.webp)
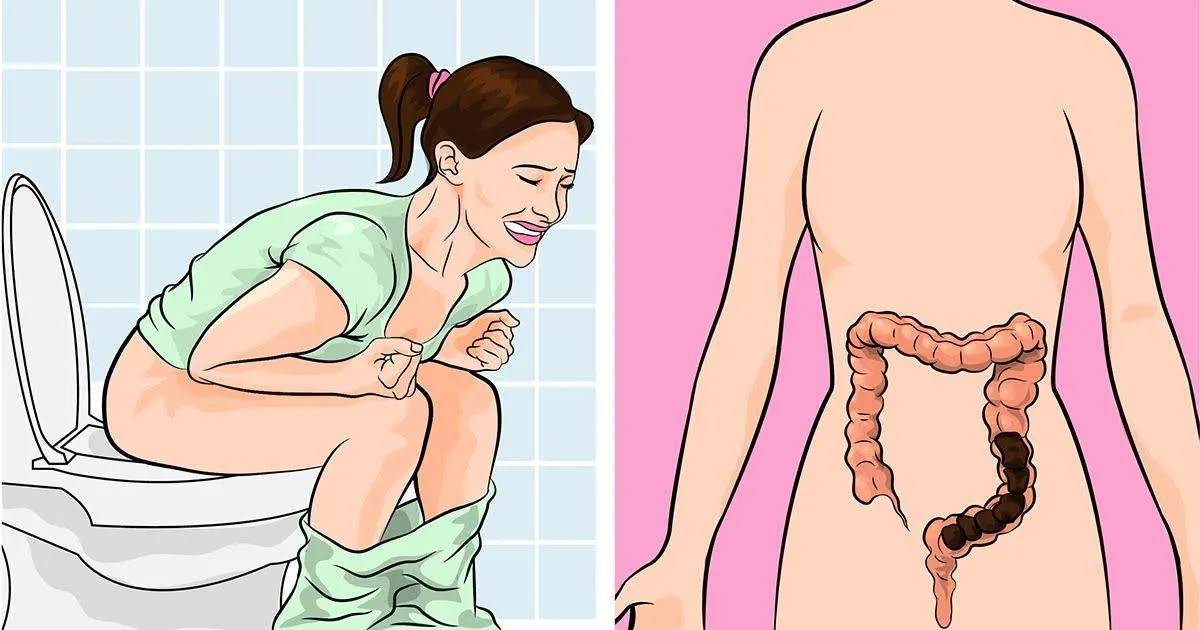
便秘是一种常见的消化道问题,可影响所有年龄层的人群。虽然很多人认为便秘只是小问题,但持续性的情况会影响生活品质,也可能暗示更严重的健康问题。不少患者在向家庭医生求助前,往往会先自行购买非处方药物;有些人甚至会在社交媒体寻求帮助,购买号称能改善便秘、效果保证的高纤饮料。也有部分人会采取更激进的方式,如进行结肠清洗,无论是通过化学方式或是未经证实的替代疗法。尽管几颗泻药看似无害,但这类药物或补充品有可能让人产生依赖,久而久之成为一有需要就依赖的快速缓解方式。对于多数上班族来说,只要这种方法仍然有效且能缓解症状,就是最好的选择。但到了最后,当他们没有其他选择,或症状长期反复却始终无解时,某些不可挽回的损害可能早已发生。
一如我以往的文章,让我来分享一些我们在肠胃科诊所经常遇到的功能性便秘的各种个案。与结肠癌相关的便秘已在另一篇文章中进行了详细论述,这里将不再对其进行详细阐述。
案例情境1
Kumar,25 岁的技术员,便秘问题已持续八个月而前来就诊。据他回忆,这一切来得突然,原本每天都有正常排便,后来却变成需要等上一周,才能勉强排出一点粪便。在这些排便间隔期间,他常感到轻微腹部不适、腹部饱胀,傍晚时腹部略显胀大,并在进食后出现腹部绞痛。而在终于能上厕所的日子里,他往往一坐就是长达三十分钟,却只能排出几颗硬块。有时即使排便后仍觉得排不尽,他会用手指尝试挖出,或用水柱冲洗直肠。然而,这些做法都无济于事,直肠内竟然异常地空空如也。他尝试过多种糖浆及药片形式的泻药,也曾每周使用一至两次灌肠,最近甚至从社交媒体上的网红推荐中购买了一种传统草本饮品。这种饮品起初似乎有效,但在过去三到四个月里,他发现自己已对它产生依赖,没有它就无法排便。他的结肠镜检查结果并无异常,目前正准备接受一系列完整的肛直肠功能与蠕动评估。
案例情境2
郑叔叔,65 岁,已退休,便秘问题已困扰他超过二十年。这段期间,他看过无数医生,做过四次结肠镜检查,尝试过各种泻药,也服用过不少非常规的补充品和草药,但始终未获得改善。他带着所有检查报告来到我的诊所,我花了将近一个小时详细了解他的症状,才发现他其实每天都会尝试上厕所。事实上,他每天都会有便意,甚至比一般人还要频繁。每当出现便意时,他都会立刻回应身体的“召唤”。他会匆忙走进厕所,坐下用力,却往往失望地发现只排出一阵气体,其他什么也排不出来。他并没有腹部不适,食欲良好,近期也没有体重下降,生活相当安逸,活动量属中等偏少。在整个访谈过程中,我注意到他一直回避提及,其实他本身是个较容易焦虑的人。进一步深入了解后,发现背后牵涉不少社会层面的问题。我建议进行一系列功能性检查,以评估肛直肠肌肉的蠕动、感觉及力量,他也非常乐意配合。结果显示,他患有所谓的直肠高敏感及排便失调。简单来说,他对排便的感觉过度敏感,同时负责排便的肌肉之间出现协调失调。
案例情境3
Linda,27 岁的年轻女性,三年来一直饱受慢性腹痛与便秘困扰,近三个月症状逐渐加重。她通常一周才上一次厕所,而每次排便往往是在出现难以忍受的腹痛和腹胀时才发生,过程中需要用力超过半小时,有时还伴随轻微的直肠出血。她尝试过多种泻药,起初确实有效,但很快就需要不断更换其他药物。近期的结肠镜检查及血液检测结果均无异常,她也不愿进行进一步的功能性检查。然而,鉴于病程长短及近期症状的频率,她的症状符合便秘型肠易激综合征。在进行详细解释与辅导后,她开始接受针对肠易激综合征的药物治疗,包括肠道选择性抗生素及益生菌。虽然她的症状已有改善,但仍需定期复诊以避免复发;若症状反复,下一步则会考虑使用神经调节类药物。
案例情境4
Pamela,30 岁的外籍女性,当时在马来西亚求学。她患有慢性便秘已超过 15 年,尝试过多种生活方式调整、增加膳食纤维摄取、服用泻药、促肠蠕动药、促分泌药物、灌肠及生物反馈治疗,但都无法长期奏效。在这段漫长的病程中,她所接受的检查比第二个案例中的郑叔叔还要多,最终被诊断为慢传输型便秘,并伴有轻微的肠易激综合征。在慢传输型便秘(也称为懒肠综合征)的情况下,Pamela 的大肠蠕动极为缓慢,平均一个月才会出现一次便意。她在家乡曾探讨过较为激进的治疗方案,包括将整个大肠切除,并把小肠与直肠直接连接,以恢复肠道的连续性。在仔细权衡各种选择后,她决定继续目前的保守治疗方式,并将这类激进的干预保留到日后再考虑。我们也与她讨论了粪菌移植的可能性,即将健康捐赠者的粪便移植到患者肠道内,希望借此恢复肠道菌群的平衡,从而缓解症状。

图一:一名由我治疗的患者正在进行粪菌移植。首先进行常规结肠镜检查,随后将处理过的粪便内容物喷洒至患者的小肠与大肠内。
粪菌移植属于费用高昂的治疗项目,并不在医疗福利或保险的保障范围内,而患者也不太愿意接受这种无法保证疗效的治疗。不过,我们也确实有其他患者在接受该治疗后预后良好,甚至无需再依赖泻药。
在分享了以上常见的临床案例后,接下来让我们进一步系统性地探讨便秘的正式医学层面,包括其成因与症状、建议的检查方式、有效的预防与管理策略,以及何时应寻求专业医疗协助。
便秘是指排便次数减少、粪便偏硬,或排便时感到疼痛,一般定义为每周排便少于三次。不过,“正常”的排便习惯因人而异,不同人之间差异很大。患有便秘的人常会形容自己的粪便硬或结块、排便时需要用力、腹胀,或排便后仍有排不尽的感觉(里急后重)。布里斯托大便分类图是一个非常实用的参考工具,可帮助医生更准确了解你的情况。看诊时,务必说明你平时的粪便形态及目前的变化情况。无论是突然或逐渐出现的变化,都有助于医生推断可能的疾病方向。
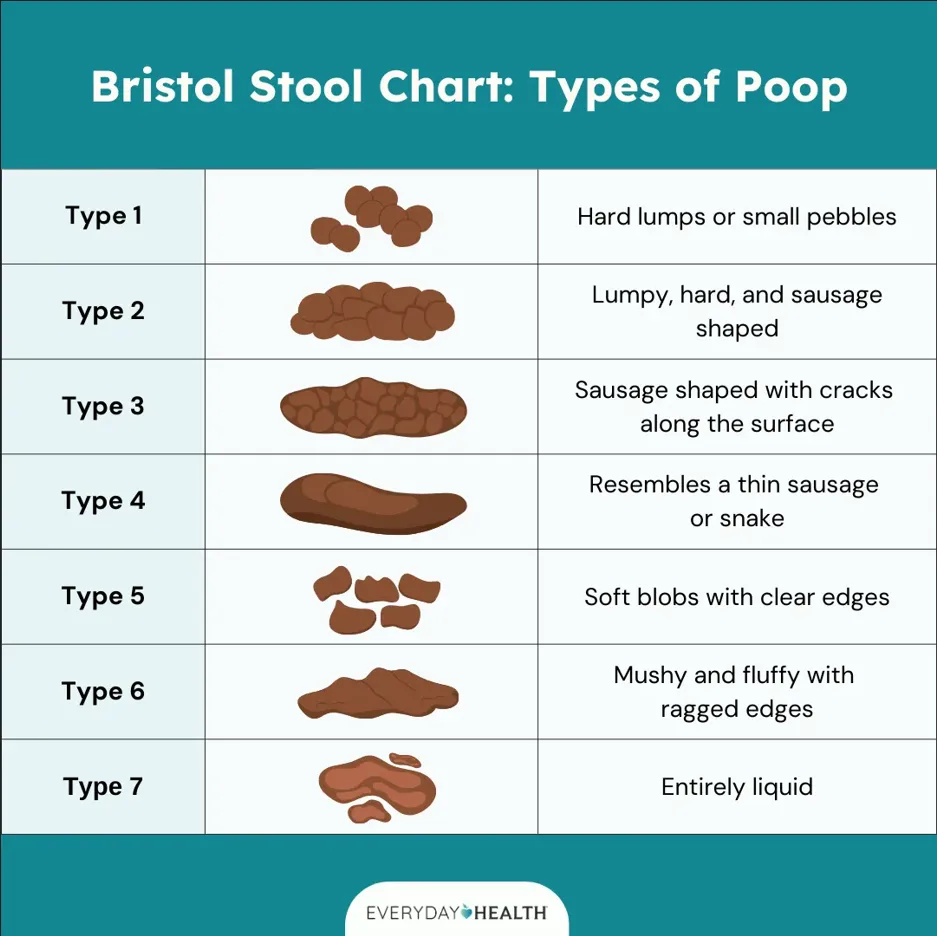
图二:正式版的布里斯托大便分类图,临床医生与护士常用来分类不同的粪便形态。相比单靠文字描述,患者通常更容易透过图像来表达自己的情况。这类标准化的大便分类图,也有助于医生之间的沟通(图片来源:Everyday Health 网站)。
图三:较为轻松且幽默的大便分类图,主要用于年轻患者,以减轻他们在诊所里的紧张与不安(图片来源:英国生物医学科学研究所)。
便秘的成因
便秘可能由以下原因引起:

图四:便秘十大常见原因的示意图。普遍认为,水分与膳食纤维摄取不足、久坐的生活方式、相关疾病及影响肠道蠕动的药物,以及肠道菌群失衡,都是造成便秘的重要因素(图片来源:gidoc.co.za 网站)。
常见症状包括:
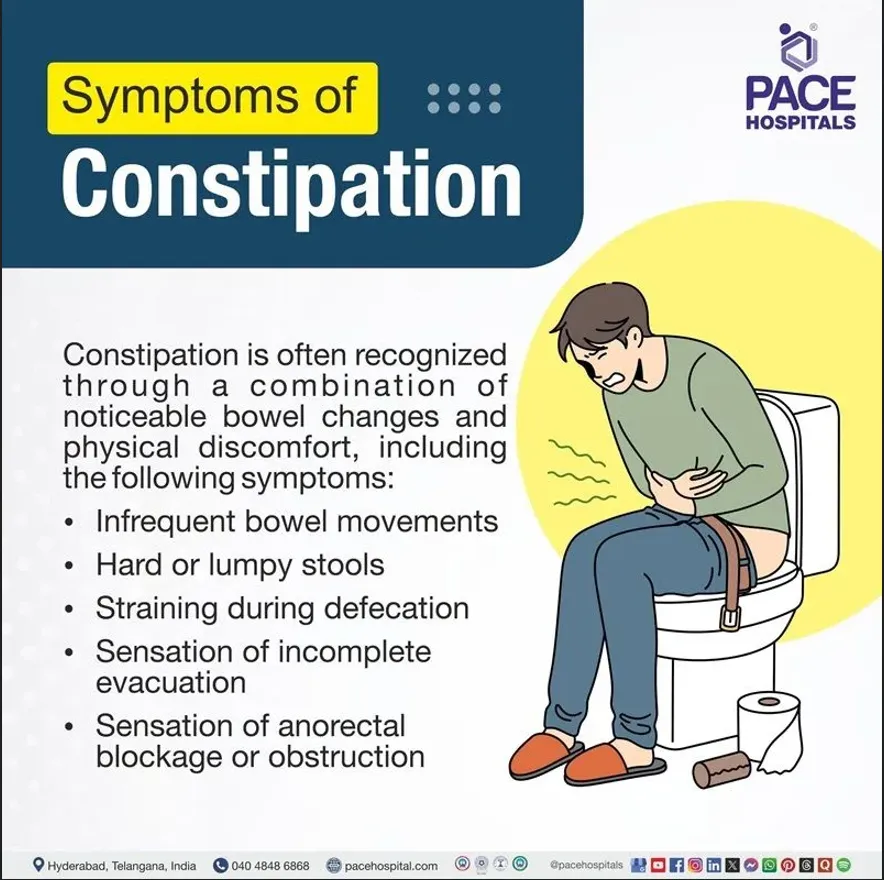
图五:便秘常见症状的示意图(图片来源:佩斯医院网站)。
虽然许多便秘情况并不需要进行大量检查,且能透过生活方式调整来改善,但在某些情况下,如症状严重、长期反复或原因不明的便秘,就有必要进一步检查。以下是医生可能采用的诊断方式:
虽然许多便秘情况并不需要进行大量检查,且能透过生活方式调整来改善,但在某些情况下,如症状严重、长期反复或原因不明的便秘,就有必要进一步检查。以下是医生可能采用的诊断方式:
病史询问与身体检查
一般情况下,医生在看诊时会先请你描述自己的症状。以下是一些事前准备的小贴士,有助于让看诊过程更有效率:
症状持续的时间 - 包括第一次出现的时间、一周的排便次数,以及与便秘发生前相比,排便频率有多大的改变。
病情进展 - 自从便秘后,排便次数是否进一步减少,以及是否需要采取额外措施才能排便。
严重程度 - 描述每次上厕所需要多久、用力的程度,是否曾用手指伸入直肠挖出粪便,或使用水柱尝试清空直肠。
其他相关症状 - 是否出现出血、排不尽的感觉、排便时有异物感,或黏液分泌。同时,也应说明是否伴随腹痛、腹部不适或腹胀,或感觉腹部有肿块。凡是你觉得不正常、且每次便秘发作时出现的情况,都建议记录下来,并在看诊时与医生讨论。例如,肠易激综合征可能会与其他功能性肠胃疾病同时存在。
生活方式调整 - 若你曾尝试改变生活习惯,也请一并说明,如增加运动量、每天饮用 2 至 2.5 公升的水、多摄取水果、膳食纤维和蔬菜,并减少红肉及加工食品的摄取,这将有助于医生作出更全面的评估。若你曾因其他疾病服用药物,请携带相关药物就诊。近期曾短期服用抗生素、止痛药或阿片类相关药物,也请主动告知,这有助于判断是否属于短暂性的便秘原因。
曾采取的措施 - 是否服用过泻药、糖浆或药片、灌肠剂或栓剂、草药或传统疗法、特殊果汁,或未经认证的补充品。若无法准确说出名称,可携带其标签或包装盒。回想服用的时间长短、如何开始使用、为何停止;若曾更换不同种类或类别的药物,说明更换原因将有助于医生日后制定治疗方案。
家族病史 - 便秘在家族中的常见性,若多位家庭成员都有类似问题,而你也已尝试过各种方法,或许需考虑肠道菌群失衡的可能性。若怀疑是功能性原因,医生也可能进一步了解你的心理及社会层面情况。请记得,焦虑和抑郁也可能影响肠道蠕动,从而导致便秘。当话题涉及这些层面时,请保持开放的心态。毕竟,我们正生活在一个节奏快、压力大的时代。
在完成详细病史询问后,医生会进行相关部位的全面身体检查。在某些情况下,肛门指诊是必要的,尤其是当你描述有直肠出血、黏液分泌、排不尽感,或排便时有异物滑出却缩回的感觉。在这些情况下,医生会温和处理,并在检查前使用充足的润滑剂。进行指诊前,医生会先检查肛门及肛周区域,并在检查后会提供纸巾或湿巾供你清洁。检查过程中,全程都会有与患者同性别的医护人员陪同。
实验室检查
医生也可能安排进一步检查,以评估是否存在相关疾病,包括:
在某些情况下,尤其是当出现警示症状或红旗征象时(可参考我之前关于结肠直肠癌的文章),医生可能会安排影像检查或内窥镜检查。

图六:一名年轻女性因急性便秘伴随严重腹痛的就诊案例。腹部与盆腔 CT 扫描显示粪便嵌塞并伴有气体影像(黄色箭头),是典型的粪便表现。患者常因剧痛而到急诊部求诊,在此之前往往已尝试多种方法,包括自行服用止痛药或泻药,甚至多次向家庭医生求助并接受止痛针治疗。
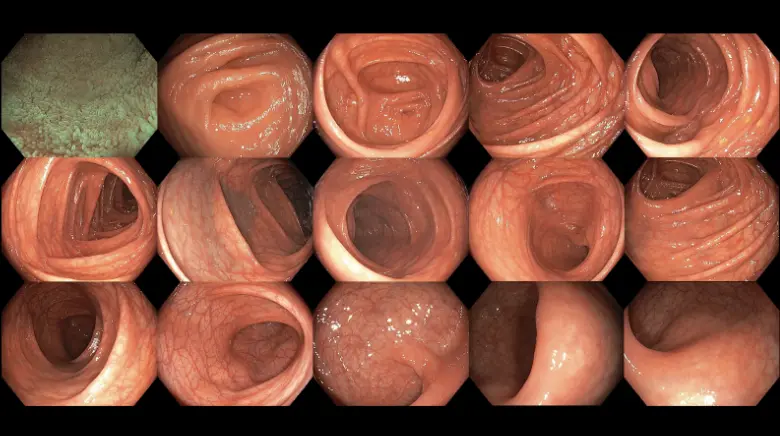
图七:结肠镜检查有助于发现结肠癌,而结肠癌也是导致慢性便秘的原因之一。
图八:Sitzmarks 胶囊检查是一种实用、安全且具成本效益的方法,可用于区分不同类型的便秘,如大肠蠕动缓慢(慢传输型便秘)或肛直肠肌肉协调失调(排便失调)。患者在服用胶囊后,五天后将进行腹部 X 光拍摄,以观察残留标记环的数量及分布情况(图片来源:Sitzmarks.com 网站)。

图九:这是我一名被诊断为排便失调患者在吞服 Sitzmarks 胶囊后第 5 天的腹部 X 光影像。可见大部分显影环集中在左侧大肠,并有部分分布于盆腔区域;右侧结肠则可见少量标记环,代表该患者可能同时患有慢传输型便秘。
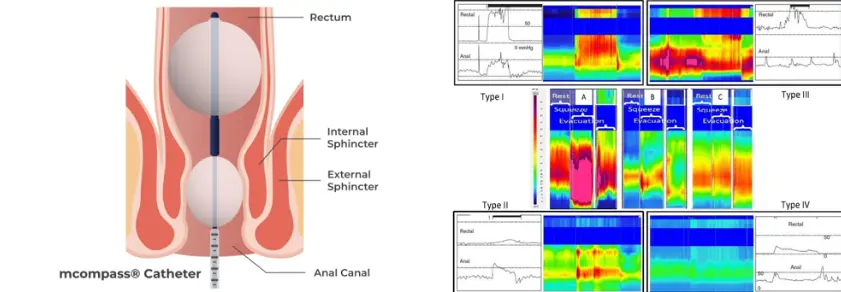
图十:肛直肠测压的检查过程(左图)及其数据分析结果(右图)。这些评估可帮助医生判断是否因直肠与肛门肌肉协调失调而导致便秘,从而制定更合适的治疗方案。(图片来源:Medspira 网站及 Lee 等,《Journal of Neurogastroenterology and Motility》,2018 年)。
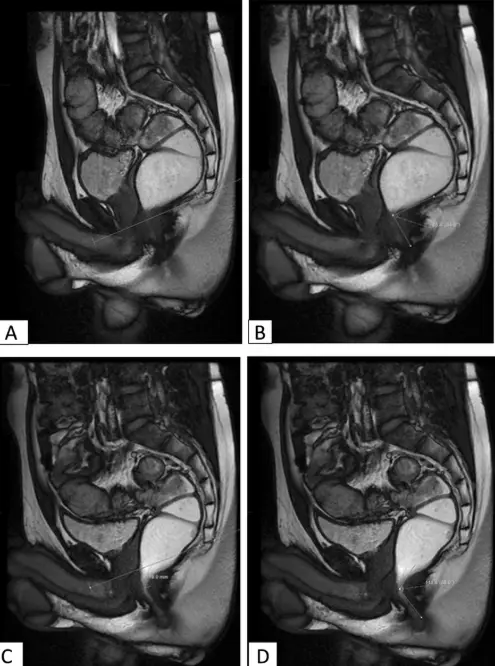
图十一:磁共振排便造影的示意图,用于评估盆底功能,并识别可能导致排便障碍的结构性或解剖异常。(图片来源:Saraya 等,《埃及放射学与核医学杂志》,2020 年)
在以下情况下,应考虑进一步检查:
未治疗的便秘可能会引发以下问题:
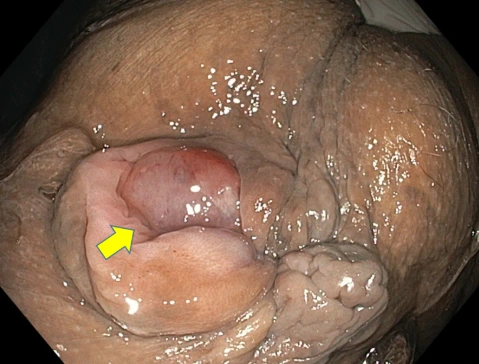
图十二:一名长期便秘患者出现脫垂性內痔(黄色箭头)。
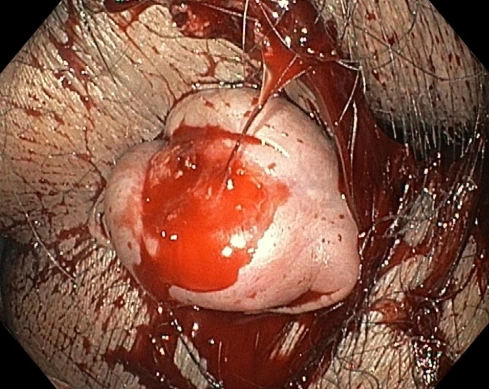
图十三:因过度用力及严重便秘而导致出血的內痔。
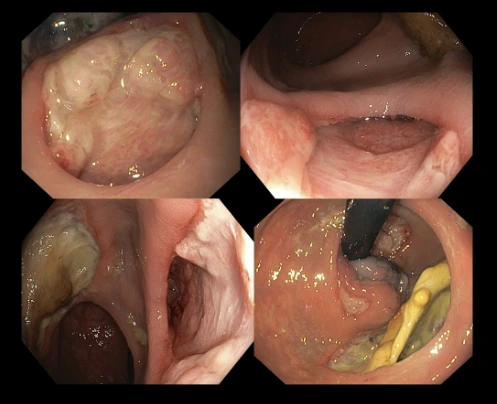
图十四:一宗在无执照机构进行、号称“非手术即可保证效果”的痔疮治疗失败案例。患者在接受该门诊治疗一周后,出现持续性的直肠分泌物、出血及剧烈疼痛的情况。结肠镜检查发现大面积溃疡,显示近期曾进行侵入性操作,而这些溃疡的位置却远离原本应处理痔疮的区域。此外,形成了瘘管,即直肠壁与肛周区域(脂肪层所在处)之间出现异常通道,导致脓液积聚及感染。通过 MRI,证实上述发现并显示该瘘管源自直肠内壁至直肠周围脂肪层的全层撕裂(穿孔)。
主要策略包括:
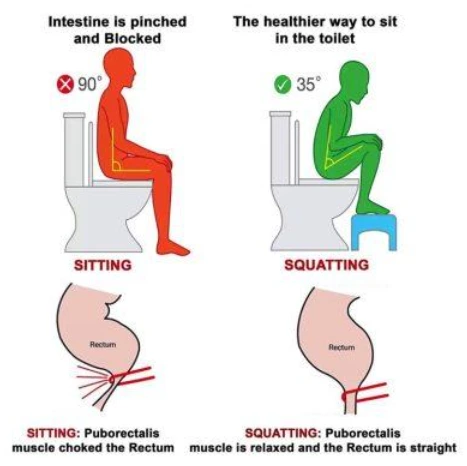
图十五:一个常被忽略、却非常实用的居家排便姿势调整方式——在坐式马桶前放置小凳子,让双脚踩高,以拉直肛直肠通道。这类姿势可透过放松耻骨直肠肌,帮助粪便顺利排出(见示意图)。(图片来源:MOTI 物理治疗网站)
若出现以下情况,应尽早就医:
医生可能会根据上述内容,建议进行进一步检查,以更全面了解并处理你的症状。
老年人因肠道蠕动减慢、同时服用多种药物及活动量减少,便秘风险较高。饮食、水分摄取、活动量及药物检视非常重要。
荷尔蒙变化及子宫增大会减慢消化过程。孕妇应在医护人员指导下,优先注重膳食纤维、水分及温和运动。
图十六:每个人都可以有自己的看法,但并非都是事实。在将某种说法当作生活方式前,应先查证可靠来源。适合某个人的方法,未必适合所有人。
便秘是一种常见,但可有效管理的消化道问题。认识其症状、了解成因,以及掌握何时与如何检查,是有效管理的关键。若症状持续或严重,应尽早寻求专业评估与治疗。养成良好生活习惯,有助于维持终身的肠道健康。

.webp?sfvrsn=20763f7d_21)
.webp?sfvrsn=f2a2c343_12)
 +604–643 8799
+604–643 8799
 请求预约
请求预约.webp?sfvrsn=276ce14_1/vector-(3).webp) 国际患者
国际患者.webp)