.webp)
Nyeri ulu hati, lebih sering dikenal dengan 'GERD' (penyakit refluks gastroesofageal) pada komunitas lokal, terjadi ketika isi dari lambung, terutama asam, kembali naik kedalam saluran makanan. Sebelum lebih lanjut, itu penting untuk mengerti beberapa kata kunci dan posisi anatomis untuk memahami penyakit umum ini.
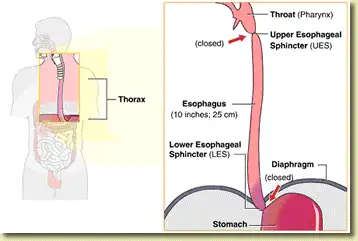
Gambar 1: Penunjuk penting pada kerongkongan, khususnya lokasi klep di bagian atas kerongkongan (UES) dan klep di bagian bawah kerongkongan(LES) (gambar milik Endoscopy Center of Monroe).
Pertama-tama, saluran makanan yang menghubungkan bagian belakang mulut kita ke lambung dikenal sebagai kerongkongan. Kerongkongan adalah tabung berotot panjang yang membantu menyalurkan makanan dan cairan ke dalam lambung. Tindakan menelan adalah tindakan yang disengaja, sedangkan pergerakan makanan ke dalam perut adalah tindakan tidak disengaja. Dua katup yang melindungi kerongkongan – klep di bagian atas kerongkongan (UES), yang terletak di bagian atas kerongkongan, dan klep di bagian bawah kerongkongan (LES), yang terletak di bagian bawah kerongkongan. Kita akan fokus terutama pada LES (Lower Esophageal Sphincter), karena ini adalah titik penting yang bertanggung jawab atas perkembangan rasa nyeri di ulu hati. Kedua klep ini terdiri dari cincin otot yang membuka dan menutup pada interval tertentu untuk memungkinkan masuknya makanan dan mencegah isi perut keluar kembali. Ketika salah satu atau kedua klep ini tidak berfungsi normal, isi lambung – baik asam maupun non-asam – akan naik kembali ke atas dan menyebabkan gejala nyeri ulu hati.
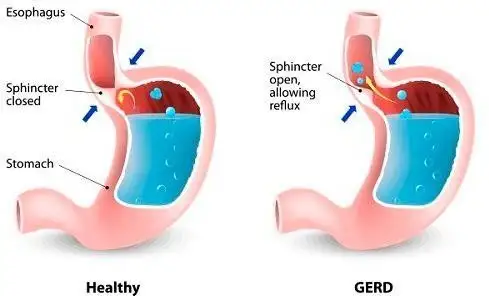
Gambar 2: Representasi diagramatik tentang fungsi klep kerongkongan bagian bawah dalam mencegah isi lambung kembali ke kerongkongan (gambar milik Health tips by Teleme).
Setelah kita mengenal bagian-bagian penting dari kerongkongan, mari kita luangkan waktu sejenak untuk memahami betapa umumnyanya rasa nyeri ulu hati (heartburn) di kalangan populasi dunia. Gejala nyeri ulu hati adalah hal yang umum, dan sekitar seperempat orang pernah mengalaminya setidaknya sekali sebulan.
Pernah mengalami kejadian tersebut sesekali bukan berarti menderita GERD, karena istilah terakhir ini dikhususkan untuk individu yang memiliki gejala lebih sering yang membutuhkan pengobatan tambahan untuk meredakan gejalanya. Nyeri ulu hati meskipun umum terjadi, dapat muncul setelah makan dalam porsi besar, terutama jika makanan tersebut digoreng dan berlemak atau setelah makan langsung berbaring. Kondisi ini juga dapat dipicu oleh obat-obatan tertentu yang merelaksasi LES lebih dari yang seharusnya. Makanan tertentu juga dapat memicu rasa terbakar di dada dengan meningkatkan keasaman isi lambung atau mengendurkan klep.
Di sisi lain, GERD adalah kondisi yang lebih tetap dan tidak mudah hilang. Sekitar seperlima populasi AS menderita GERD, terutama karena faktor risiko terkait seperti obesitas, merokok, dan konsumsi alkohol. Faktor risiko lain yang memicu GERD meliputi jenis kelamin laki-laki dan usia di atas 50 tahun. Di Malaysia, dilaporkan bahwa sekitar 10% pasien mengalami nyeri ulu hati setiap bulan, sedangkan 6% akan mengalami gejala mingguan. Berdasarkan kumpulan data yang diterbitkan hampir dua dekade yang lalu, angka prevalensinya sudah dianggap tinggi di negara kita. Dengan meningkatnya tren obesitas yang melanda Malaysia dan fakta bahwa obesitas merupakan faktor risiko yang terkenal dapat menyebabkan nyeri ulu hati dan GERD, kita hanya bisa membayangkan bagaimana kejadiannya telah meningkat secara eksponensial selama bertahun-tahun.
Menariknya, sebuah studi berbasis komunitas menemukan bahwa etnis mungkin berperan dalam prevalensi nyeri ulu hati, dengan dikatakan bahwa orang India mengalami lebih banyak gejala dibandingkan dengan orang Tionghoa dan Melayu. Penyebab paling mungkin dari perbedaan tersebut masih menjadi perdebatan. Namun, faktor lingkungan lokal, seperti norma budaya, praktik sosial, kebiasaan makan, dan pilihan gaya hidup, dapat memainkan peran penting.
Gejala klasik nyeri ulu hati dimulai dengan sensasi terbakar di bagian atas perut yang dikenal sebagai epigastrium. Sensasi terbakar kemudian menjalar ke bagian tengah dada, di mana pasien mungkin menggambarkan sensasi sesak dada, nyeri dada, dan perasaan kesulitan dalam menarik napas dalam-dalam.
Gejala lain yang mungkin menyertainya termasuk meningkatnya produksi air liur (dikenal sebagai water brash), rasa asam di bagian belakang tenggorokan (acid brash), tenggorokan kering, iritasi tenggorokan, sakit tenggorokan, batuk berkepanjangan, dan bau mulut. Gejala nyeri ulu hati sering terjadi setelah mengonsumsi makanan berat, terutama yang kaya lemak dan protein, dan diperparah saat langsung berbaring setelah makan. Perut yang terlalu penuh membuat isinya jauh lebih mudah dimuntahkan kembali ke kerongkongan, sehingga memperburuk gejala GERD. Oleh karena itu, salah satu saran umum yang diberikan untuk mengurangi rasa panas di dada adalah dengan makan dalam porsi kecil dan sering, menghindari makan empat jam sebelum tidur, menyangga bagian kepala tempat tidur saat tidur, dan berbaring miring ke kiri agar gravitasi menarik isi perut menjauh dari LES (Lower Esophageal Sphincter).
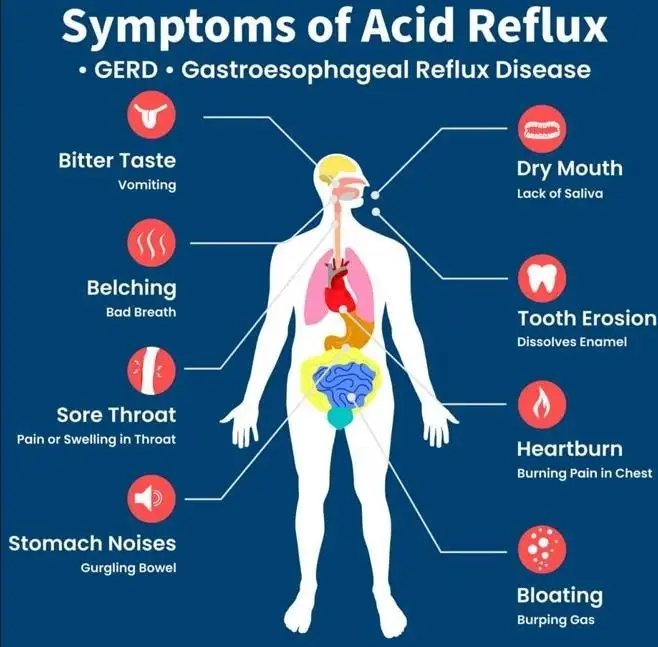
Gambar 3: Gejala dan tanda nyeri ulu hati dalam ilustrasi kartun (Gambar milik situs web Australia Wide First Aid)..
Nyeri ulu hati yang parah dan kronis juga dapat menyebabkan karies gigi, masalah sinus, dan bahkan infeksi telinga tengah (otitis media). Beberapa pasien bahkan mungkin merasakan benjolan atau rasa sesak di tenggorokan mereka dan gagal mengeluarkannya melalui batuk dan muntah. Sensasi tegang ini dikenal sebagai 'globus pharyngeus', atau singkatnya globus, dan diyakini disebabkan oleh otot-otot yang tegang di sekitar tenggorokan.
Sensasi nyeri ulu hati (heartburn) umumnya dikaitkan dengan kondisi yang disebut dispepsia fungsional, di mana pasien mengalami rasa kenyang lebih awal atau perasaan penuh terlalu cepat selama makan. Mereka juga bisa mengeluh sering bersendawa, perut kembung, rasa tidak nyaman di perut, dan sering merasa dada dan perut terasa berat. Dispepsia fungsional pada kategori ini dari hasil pasien dari kegagalan otot lambung untuk rileks dan mengakomodasi makanan yang masuk, sehingga meningkatkan kemungkinan refluks asam (naiknya isi lambung) Mual dan muntah sangat jarang terjadi pada kasus nyeri ulu hati dan dispepsia fungsional dan biasanya menunjuk pada masalah lain bersamaan.
Penting untuk dicatat bahwa gejala-gejala tertentu memerlukan perhatian medis segera dalam kasus nyeri asam lambung. Gejala-gejala ini termasuk dalam kategori gejala peringatan dini dan meliputi kesulitan dan nyeri saat menelan (disfagia dan odinofagia), penurunan berat badan dan nafsu makan, muntah darah, dan keluarnya darah dalam tinja. Jika Anda mengalami salah satu gejala ini, jangan ragu untuk mencari pertolongan medis. Kesehatan dan kesejahteraan Anda adalah prioritas utama kami, dan kami di sini untuk membantu Anda mengatasi tantangan-tantangan ini.


Gambar 4: Minuman berkafein, teh tertentu, alkohol, cokelat, dan produk kakao dapat menyebabkan gejala nyeri ulu hati. Waspadai juga jenis zat tambahan yang Anda masukkan ke dalam minuman yang tampaknya tidak berbahaya dan bebas dari rasa panas di dada, karena ada senyawa tertentu yang masih dapat meningkatkan produksi asam, mengiritasi lapisan kerongkongan, dan mengendurkan klep kerongkongan bagian bawah.
Sebagian besar pasien yang menderita nyeri ulu hati terus-menerus seringkali menyadari makanan tertentu yang memicu gejala mereka dan berusaha sebaik mungkin untuk mengurangi atau menghilangkannya dari makanan mereka. Makanan dan minuman ini meliputi kopi dan beberapa jenis teh berkafein, cokelat, alkohol, produk kakao, minuman berkarbonasi, tomat, makanan berlemak atau pedas, dan buah-buahan sitrus (seperti jeruk, nanas, mandarin, jeruk keprok, jeruk nipis, lemon, belimbing, dan jeruk bali). Kafein adalah zat yang dikenal dapat menyebabkan nyeri dengan cara merelaksasi LES (Lower Esophageal Sphincter) dan juga meningkatkan produksi asam lambung. Kopi sendiri secara alami bersifat asam dan dapat mengiritasi lapisan kerongkongan, yang berada dalam lingkungan basa.
Teh berbahan dasar mint, seperti spearmint dan peppermint, juga bekerja melalui mekanisme serupa dengan merelaksasi klep kerongkongan bagian bawah (LES), sehingga meningkatkan kemungkinan refluks asam. Terkadang, bukan hanya tehnya saja, karena pilihan teh dengan rasa asam lemah sangat banyak – mungkin hanya pilihan menambahkan sepotong lemon, sedikit daun mint, atau potongan gula yang perlu dihindari. Memiliki panduan makanan mengenai pemicu nyeri ulu hati yang umum dikenal dapat membantu pasien membuat pilihan yang tepat tentang makanan sehari-hari mereka. Namun, beberapa individu mungkin lebih rentan terhadap makanan lain yang tidak tercantum di sini.

Gambar 5: Menghindari buah-buahan sitrus dan asam, makanan pedas, berlemak, dan berminyak membantu mengurangi dan mencegah gejala nyeri ulu hati, dan dalam kasus GERD, penghindaran makanan tersebut mengurangi kejadian kambuhnya nyeri ulu hati.
Setelah menjelaskan jenis makanan yang perlu dikurangi atau dihindari, kita juga perlu mempertimbangkan gaya memasaknya. Terlepas dari etnisnya, orang Malaysia umumnya menyukai makanan pedas dan berlemak. Makanan yang digoreng, digoreng dua kali, rendang, kari, atau bahkan hidangan yang diolah dengan banyak bawang bombai dan bawang putih dapat memicu serangan nyeri ulu hati. Selain bersifat asam (seperti bawang bombai dan bawang putih), makanan berminyak dan berlemak lebih lama berada di usus dan membutuhkan waktu lebih lama untuk dicerna. Diet tinggi 'oligosakarida, disakarida, monosakarida, dan poliol yang mudah difermentasi' (atau diet FODMAP) adalah kelas senyawa makanan lain yang sulit diserap di usus kecil sehingga menyebabkan fermentasi dan pembentukan gas.
Akibatnya, pasien akan mengalami gejala kembung dan perut bergas, yang terkadang dapat menyebabkan perut kembung dan memperburuk frekuensi serta tingkat keparahan nyeri ulu hati. Contoh makanan dengan kandungan FODMAP tinggi antara lain bawang bombai dan bawang putih. Namun, tidak disarankan untuk sepenuhnya menerapkan diet FODMAP tanpa terlebih dahulu berkonsultasi dengan dokter, karena diet ini bukanlah bagian resmi dari penanganan nyeri ulu hati dan GERD.
Beralih dari topik kuliner ke pilihan gaya hidup dan aktivitas yang dapat menyebabkan nyeri ulu hati, pasien terus-menerus disarankan untuk menurunkan berat badan, berhenti merokok, dan mengonsumsi alkohol dalam jumlah sedang.
Era kehidupan modern, nanoteknologi, kecerdasan buatan, dan, dalam waktu dekat, peningkatan penggunaan robot sebagai pendukung telah membuat segalanya jauh lebih nyaman. Dengan menekan sebuah tombol atau hanya menggeser sakelar, operasi di bidang apa pun dapat diselesaikan hanya dalam hitungan detik. Ditambah dengan banyaknya ketersediaan makanan olahan yang menyebabkan kurangnya aktivitas fisik dan kelebihan nutrisi, tidak mengherankan jika secara global kita sedang menghadapi pandemi obesitas. Hidup jelas lebih mudah!
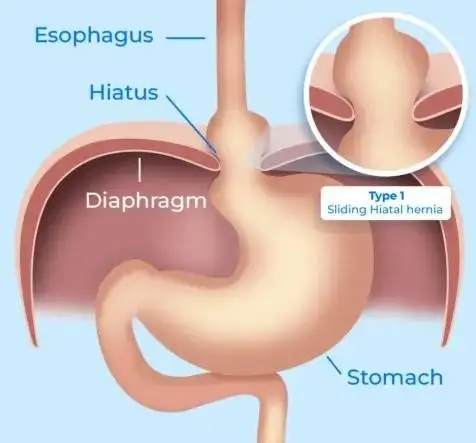
Gambar 6: Otot diafragma memainkan peran sentral dalam aparatus otot LES – diafragma yang lemah meningkatkan kemungkinan terbentuknya hernia hiatus. Kartun ini menunjukkan pergerakan bagian atas lambung ke dalam rongga dada, di atas diafragma (gambar milik situs web Dr. Gabriel Arevalo MD).
Kelebihan berat badan atau obesitas meningkatkan lingkar perut dan tekanan intra-abdominal, yang akibatnya membatasi kemampuan lambung untuk mengembang dan berpotensi menurunkan ambang batas aliran balik kandungan asam ke kerongkongan. Jika suatu isi tidak dapat bergerak maju, maka isi tersebut akan bergerak mundur dan mengikuti jalur yang paling mudah dilalui. LES (Lower Esophageal Sphincter), yang kini menghadapi peningkatan tekanan perut, semakin melemah, memungkinkan bagian atas perut untuk menggulung ke atas ke dalam rongga dada, di atas diafragma (otot yang memisahkan dada dari perut dan memainkan peran penting dalam membentuk aparatus otot LES), sehingga menciptakan apa yang dikenal sebagai hernia hiatus. Hambatan yang diciptakan oleh LES kini telah hilang. Bagian atas lambung, yang diketahui mengandung sel-sel penghasil asam (sel parietal), akan dengan bebas membasahi bagian bawah kerongkongan dengan asam, sehingga semakin meningkatkan risiko, keparahan, dan kemungkinan komplikasi dari mulas dan GERD.

Gambar 7: Dampak merokok dan konsumsi alkohol sangat besar dalam mekanisme utama memperburuk gejala nyeri ulu hati, memicu GERD, dan meningkatkan risiko komplikasi terkait GERD seperti esofagitis, esofagus Barrett, dan kanker kerongkongan (gambar milik situs web City of Hope).
Merokok meningkatkan risiko nyeri ulu hati dengan semakin merelaksasi LES, merangsang produksi asam lambung yang lebih banyak, dan mengurangi produksi air liur, yang mana produksi air liur sangat penting dalam menetralkan asam lambung. Bersama dengan UES dan LES, air liur merupakan mekanisme pertahanan bawaan terhadap refluks asam. Merokok dapat merusak kelenjar ludah, sementara nikotin dapat meningkatkan viskositas air liur yang dihasilkan, sehingga mengurangi aliran air liur yang memadai. Ketika hal ini terjadi, produksi air liur menurun dan
air liur yang mengental tidak lagi dapat menjalankan fungsinya secara optimal, sehingga mencegah seseorang untuk mengeluarkan asam lambung yang dimuntahkan melalui proses menelan.
Konsumsi alkohol juga dapat memicu gejala yang berhubungan dengan mulas, sama seperti merokok. Namun menariknya, ada mekanisme tidak langsung yang dapat memperburuk keadaan lebih lanjut ketika konsumsi alkohol dilakukan secara berlebihan. Seringkali, alkohol tidak hanya dikonsumsi sendiri tetapi juga dikombinasikan dengan camilan atau makanan goreng/berminyak untuk menunda pengosongan lambung dan, dengan demikian, memperlambat penyerapan alkohol dan efek mabuk. Bahkan koktail, atau campuran minuman beralkohol yang kini menjadi favorit di kalangan masyarakat, dicampur dengan soda (minuman berkarbonasi) dan gula, yang, seperti yang telah dijelaskan di atas, dikenal sebagai pemicu nyeri ulu hati.
Mengingat bahwa pilihan diet dan gaya hidup dapat memengaruhi baik nyeri ulu hati maupun GERD, sangat penting untuk mengedukasi pasien bahwa perubahan yang lambat namun progresif, seperti penurunan berat badan melalui aktivitas fisik, modifikasi diet, berhenti merokok, dan menjauhi alkohol, sangat bermanfaat.
Pemeriksaan terkait GERD terutama melibatkan endoskopi saluran pencernaan bagian atas, juga dikenal sebagai endoskopi, untuk mencari hernia hiatus terkait, komplikasi seperti peradangan kerongkongan, esofagus Barrett, dan kanker stadium awal atau lanjut.
Endoskopi juga dapat membantu mengidentifikasi masalah penyerta lainnya, seperti infeksi Helicobacter pylori, tukak lambung dan duodenum, serta kanker lambung.
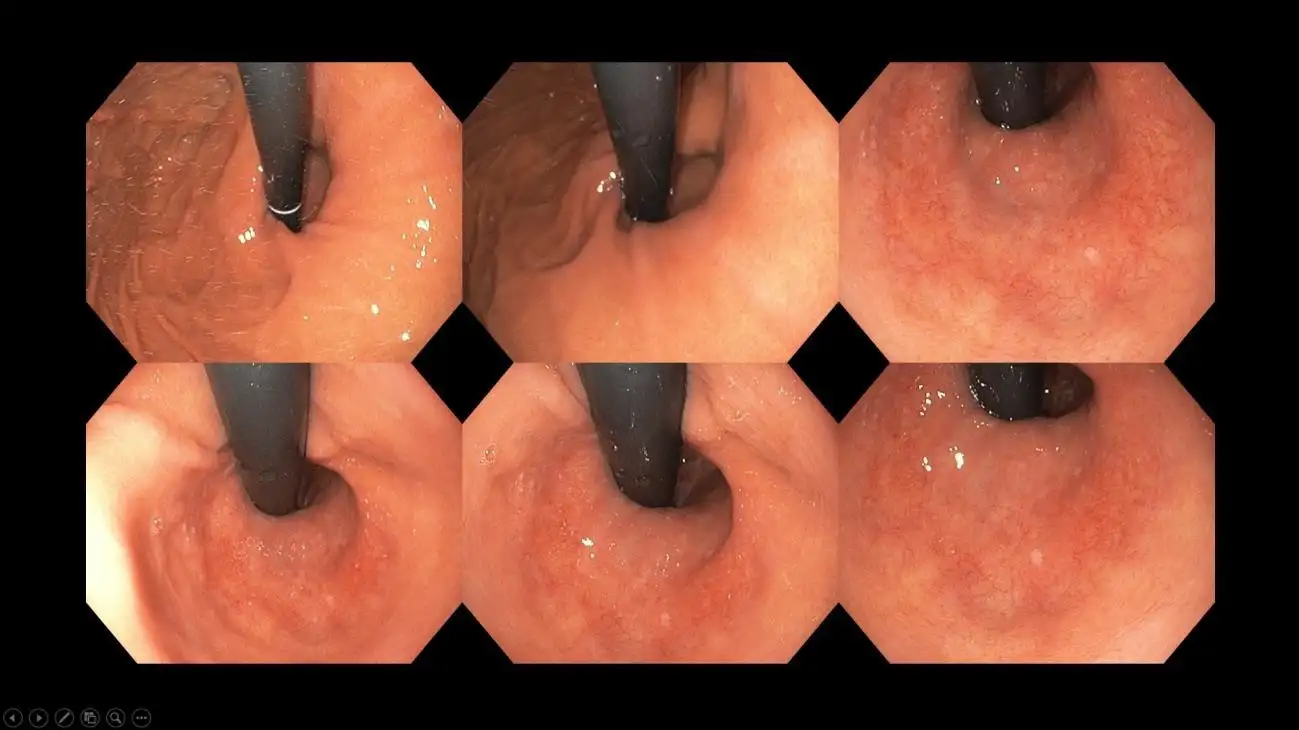
Gambar 8: Penampakan hernia hiatus – perhatikan lubang menganga besar yang mengelilingi tabung hitam yang merupakan endoskop – LES yang kompeten seharusnya menelan endoskop sehingga tidak menyisakan celah atau hanya celah minimal di antaranya.
Gambar 9: Ulkus inflamasi pada bagian bawah kerongkongan akibat nyeri ulu hati kronis – temuan ini disebut esofagitis refluks dan diklasifikasikan berdasarkan panjang ulkus dan keterlibatan melingkar untuk memandu pemilihan agen penekan asam selanjutnya.
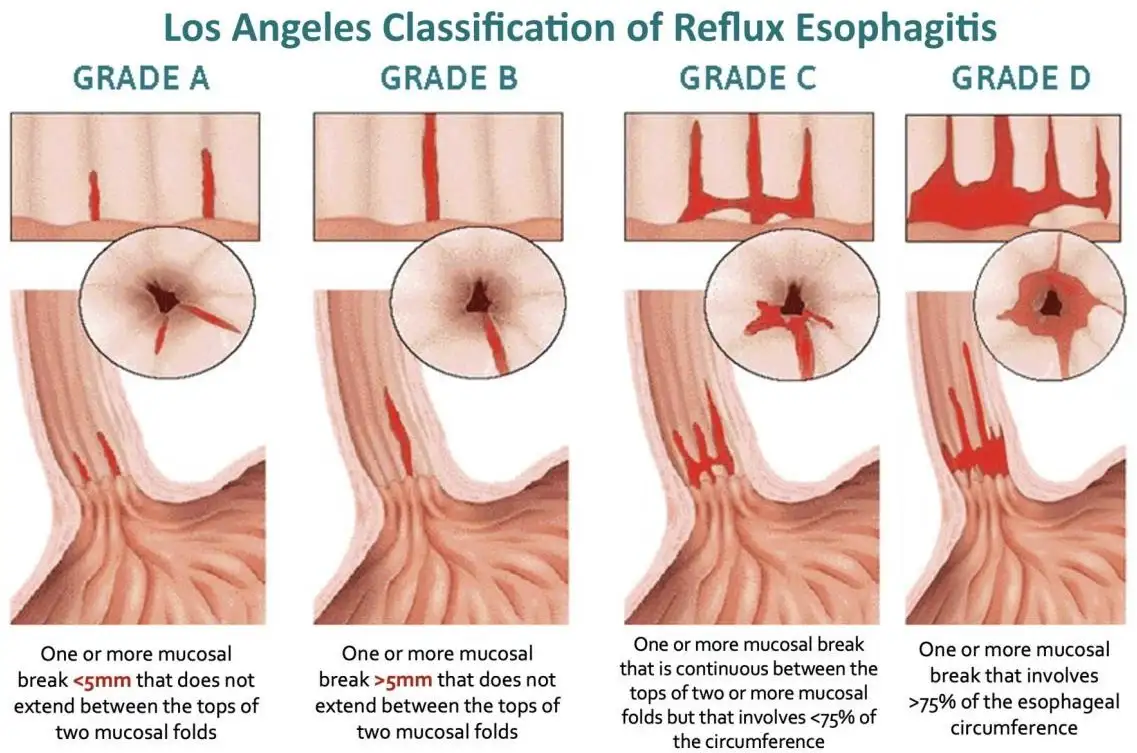
Gambar 10: Berbagai tingkatan esofagitis refluks – dokter memberikan perhatian khusus pada temuan endoskopi ini dan melaporkannya sesuai dengan itu. Temuan tersebut bermanfaat untuk meningkatkan pemahaman tentang tingkat keparahan GERD yang mendasarinya, pemilihan pengobatan, evaluasi respons terhadap pengobatan (baik melalui pemantauan gejala atau pengulangan endoskopi) dan konseling pasien.
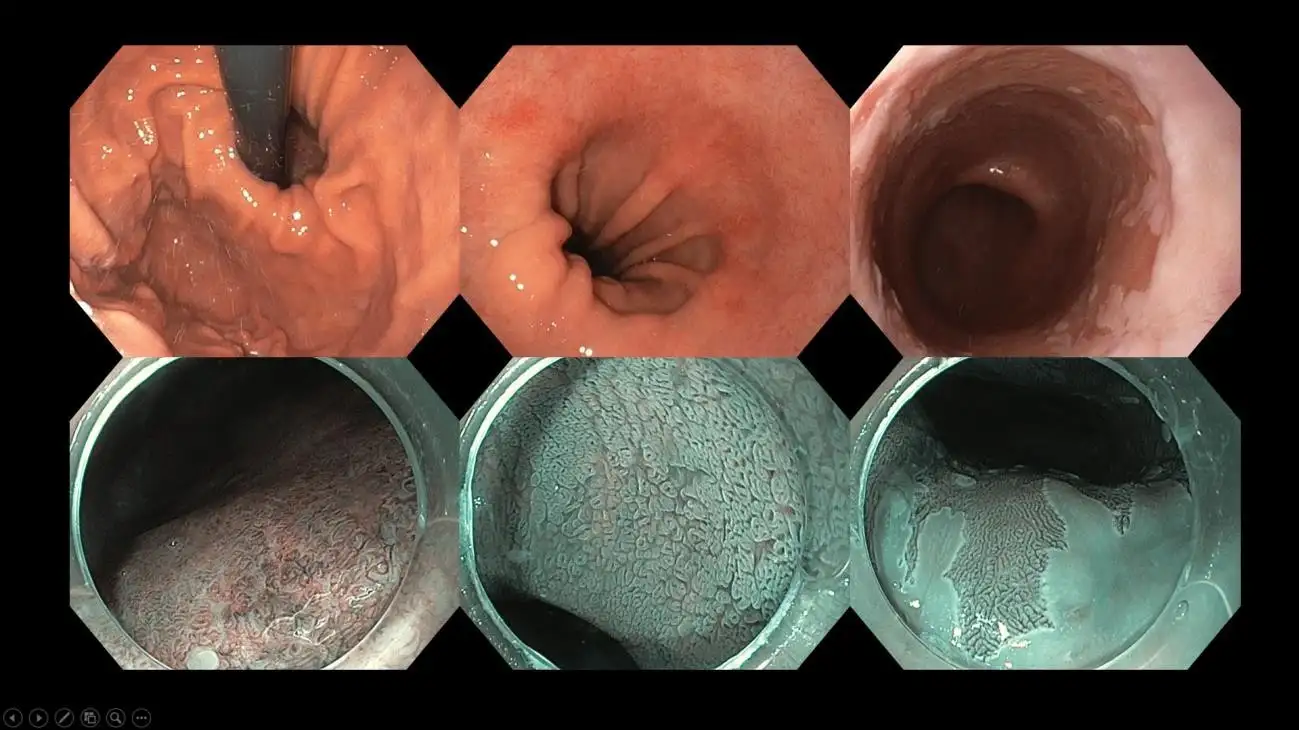
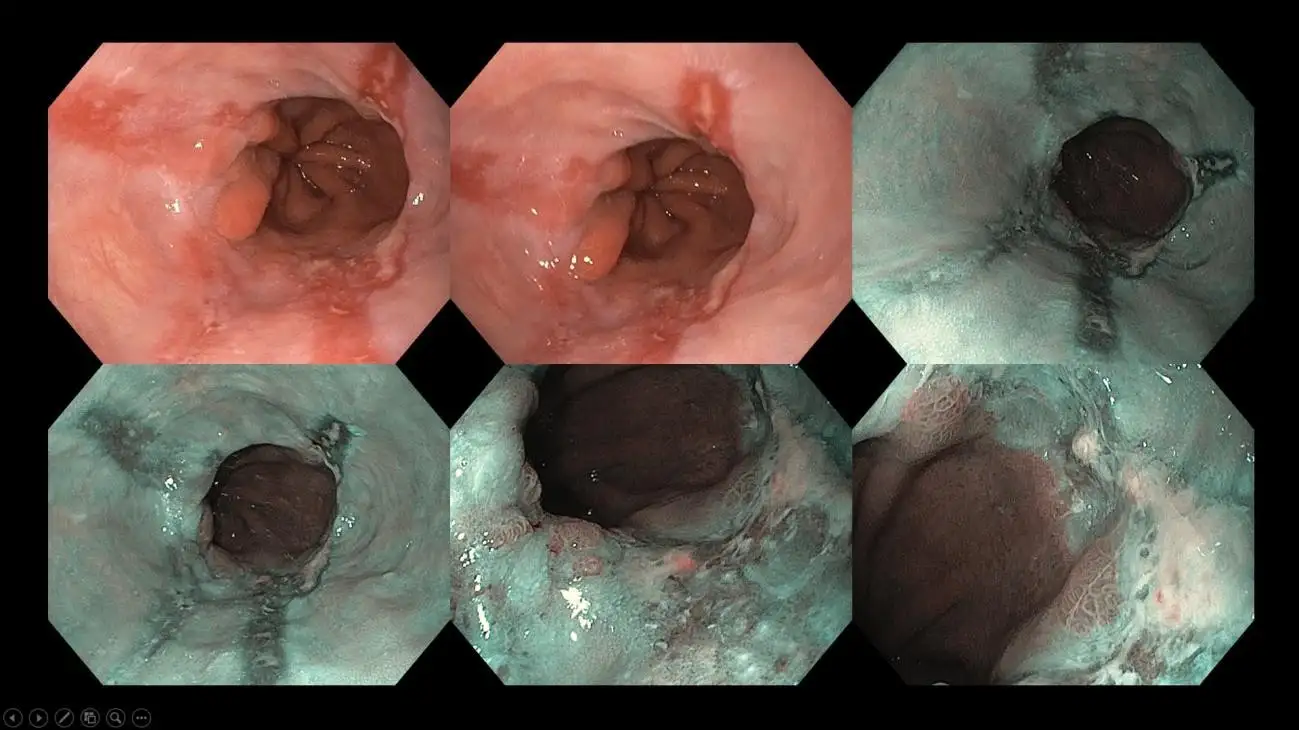
Gambar 11: Seorang pasien dengan hernia hiatus besar dan esofagus Barrett – lapisan khusus pada kerongkongan yang menandakan potensi risiko berkembang menjadi kanker kerongkongan. Di pusat pencitraan canggih seperti kami, kami melakukan endoskopi dengan peningkatan citra dan kromoendoskopi berbasis pewarna dengan endoskop beresolusi tinggi untuk menggambarkan secara cermat luasnya esofagus Barrett dan mencari area mencurigakan yang memerlukan biopsi dan mungkin, pengangkatan endoskopi. Beberapa area di dalam lapisan Barrett mungkin mengandung perubahan kanker stadium awal, dan modalitas pencitraan ini membantu ahli endoskopi untuk menargetkan area tersebut dengan tepat.
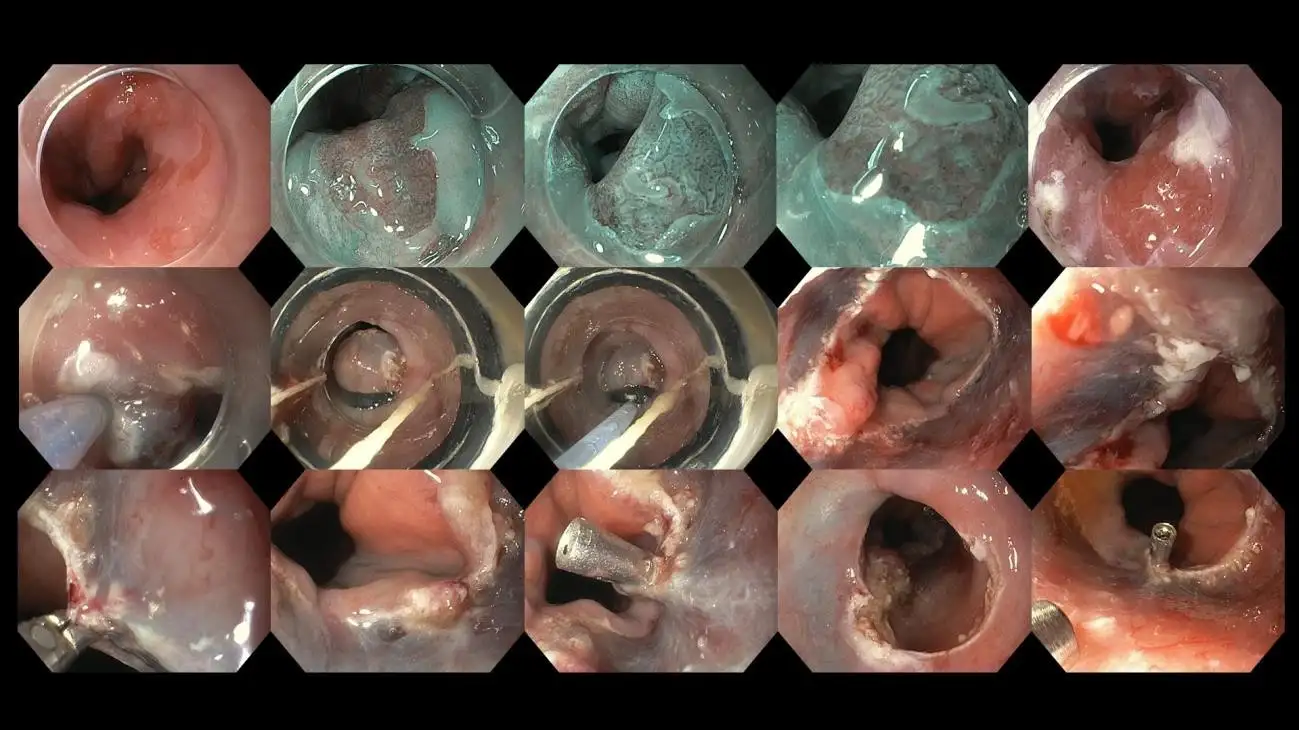
Gambar 12: Kasus pasien dengan esofagus Barrett yang ditemukan memiliki perubahan prakanker selama evaluasi pencitraan canggih yang detail, saat ini sedang menjalani reseksi/eksisi endoskopi. Terapi endoskopi bermanfaat untuk kanker stadium awal yang belum menginvasi kedalam lapisan yang lebih dalam dari dinding kerongkongan karena menawarkan kesembuhan tanpa pengobatan tambahan.
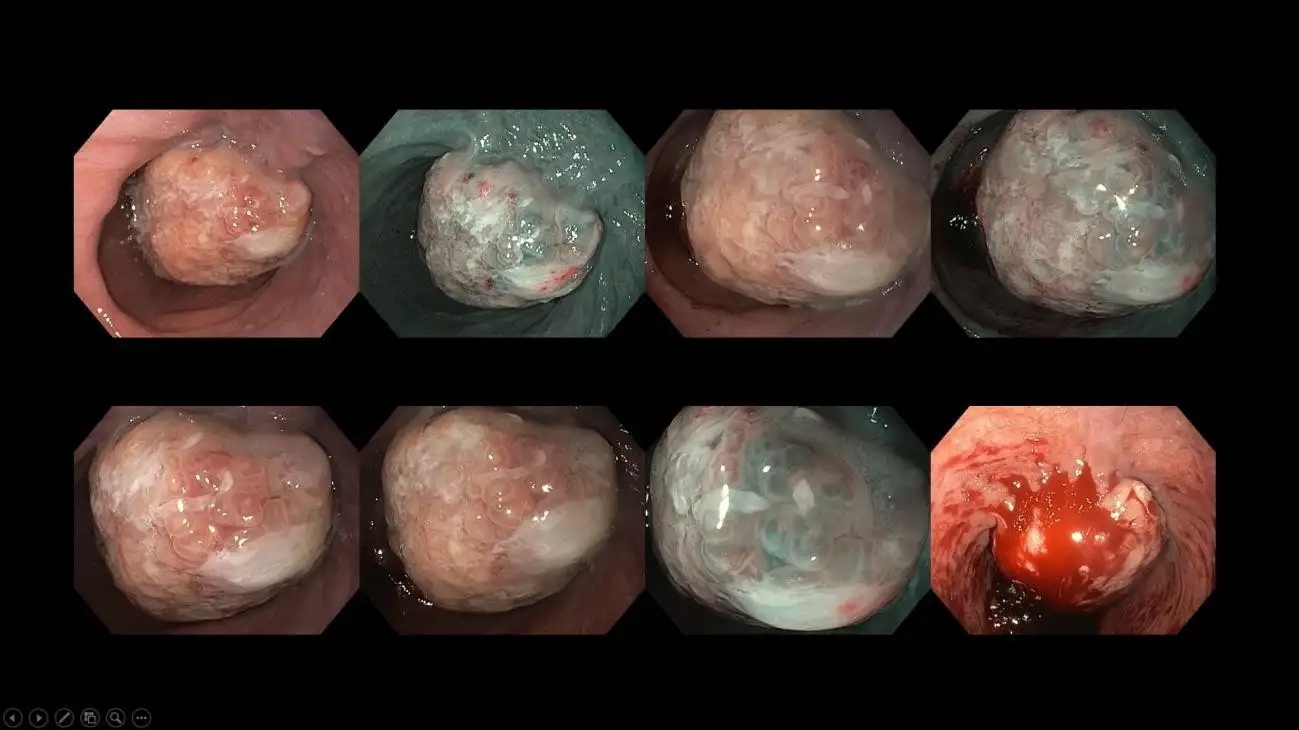
Gambar 13: Kasus kanker kerongkongan stadium lanjut yang timbul dari riwayat gejala nyeri ulu hati kronis. Kasus seperti itu memerlukan pemindaian CT lanjutan untuk mencari penyebaran metastasis, diikuti dengan konsultasi bedah dan onkologi. Seringkali, diskusi dewan multidisiplin akan diadakan untuk pasien-pasien ini guna membahas manajemen yang disesuaikan untuk memberikan perawatan dan hasil yang paling optimal bagi mereka.
Pemeriksaan yang lebih detail untuk GERD melibatkan pemantauan pH kerongkongan selama 24 jam dan studi impedansi. Di sini, sebuah tabung tipis dan fleksibel dimasukkan melalui hidung Anda dan diposisikan di atas klep kerongkongan bagian bawah (LES) untuk menganalisis tingkat keparahan dan frekuensi episode refluks. Pasien akan mengenakan alat kecil di ikat pinggang atau pinggang mereka, yang mana alat tersebut akan menyimpan semua data yang direkam. Di akhir pengujian, kawat dilepas dari hidung, dan data diunggah ke komputer khusus dengan aplikasi khusus untuk menginterpretasikan hasilnya. Perangkat nirkabel yang lebih modern, seperti perangkat penguji pH Bravo, juga tersedia, di mana perekam dipasang sementara di ujung bawah kerongkongan. Pemantauan pH menawarkan modalitas yang lebih akurat untuk mendiagnosis GERD yang sebenarnya, karena ada varian lain dari gangguan terkait nyeri ulu hati yang perlu dipertimbangkan, seperti penyakit refluks non-erosif (NERD), hipersensitivitas esofagus, dan nyeri ulu hati fungsional, suatu varian dari gangguan interaksi usus-otak (DGBI).
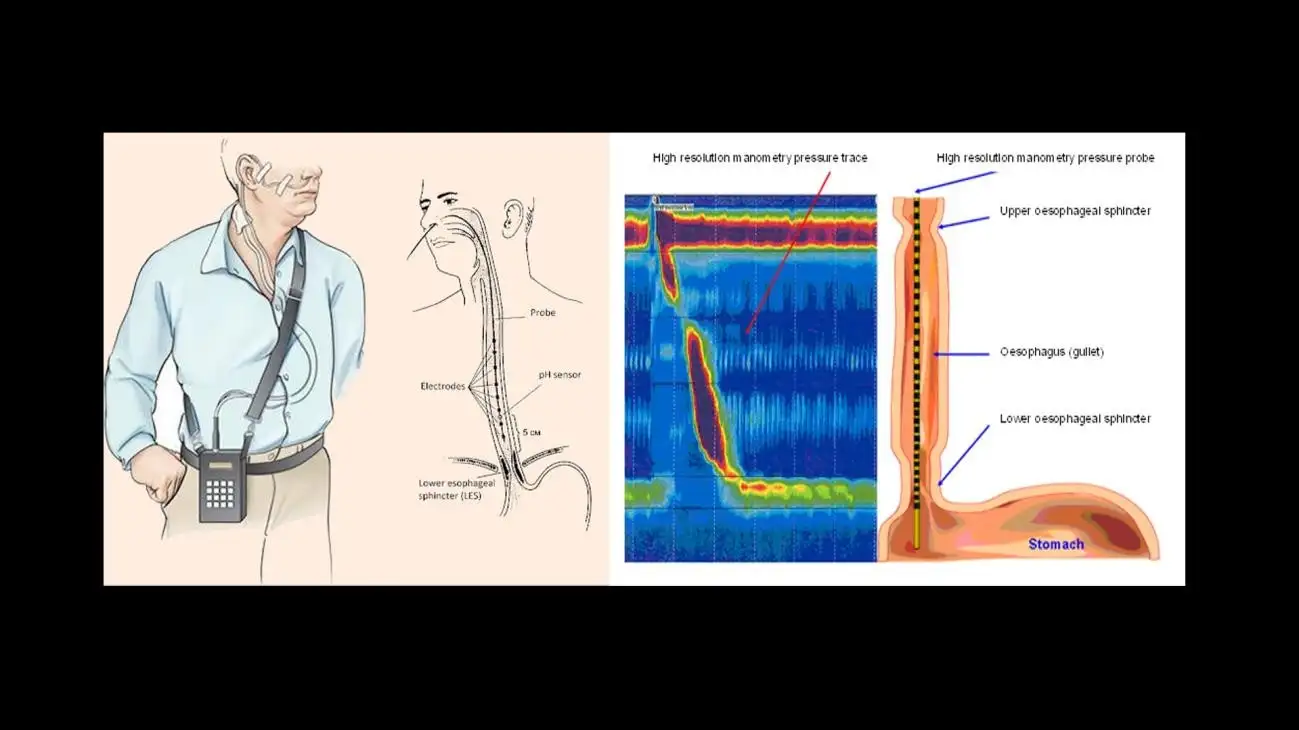
Gambar 14: Ilustrasi gambar pemantauan pH ambulatori 24 jam (kiri) dan manometri esofagus resolusi tinggi (kanan) (gambar milik situs web Srushti Gastro & Liver Clinic dan Hull University Teaching Hospitals).
Dalam kebanyakan kasus, manometri esofagus resolusi tinggi juga akan dilakukan dalam pengaturan serupa sebelum studi pH sebagai cara untuk merekam integritas, tekanan, dan pergerakan kerongkongan dan klepnya. Tes manometri dilakukan untuk menyingkirkan kemungkinan adanya gangguan pergerakan kerongkongan atau penyebab sekunder yang dapat memicu rasa terbakar di dada. Baik tes pH maupun manometri sangat penting dalam menegaskan diagnosis yang tepat dari GERD sejati dibandingkan dengan gangguan kerongkongan lainnya, karena penanganannya sangat berbeda. Hal ini menjadi lebih relevan lagi ketika pembedahan dipertimbangkan untuk GERD yang sulit diobati. Anda ingin memastikan bahwa tujuan pembedahan benar-benar untuk GERD yang resisten terhadap pengobatan dan bukan sesuatu yang lain yang memerlukan bentuk penanganan yang berbeda.
Metode lama untuk mendiagnosis GERD, seperti pemeriksaan barium swallow, kini jarang digunakan dan terbatas pada pusat-pusat yang tidak memiliki akses ke pemeriksaan pH dan manometri.
Penanganan nyeri ulu hati merupakan kombinasi dari modifikasi gaya hidup dan pengobatan. Seringkali, pasien lebih cenderung meredakan serangan mulas mereka dengan obat-obatan yang dijual bebas karena alasan kenyamanan dan agar mereka dapat terus menjalani gaya hidup yang sibuk. Namun, ada baiknya untuk mundur selangkah dan merenungkan diskusi di atas, memeriksa faktor risiko yang saling terkait yang dapat memperburuk nyeri ulu hati, daripada hanya mengandalkan obat-obatan.
Berikut ringkasan penanganan non-farmakologis yang saya sarankan kepada pasien saya:
Berikut adalah daftar pilihan pengelolaan farmakologis untuk mendukung perubahan gaya hidup dan pola makan yang berkelanjutan.
Penanganan nyeri ulu hati dan GERD melalui pembedahan dan metode endoskopi terbaru berada di luar cakupan diskusi ini dan akan dibahas dalam artikel terpisah di masa mendatang.
Namun, perlu dicatat bahwa komplikasi GERD, dan khususnya esofagus Barrett serta kanker esofagus yang berasal dari jaringan esofagus khusus ini, tidaklah jarang terjadi seperti yang diperkirakan sebelumnya. Spektrum penyakit ini meningkat di Malaysia karena obesitas dan gangguan metabolisme terkait lainnya. Jadi, jika Anda mengalami gejala mulas yang berkepanjangan dan ketidaknyamanan yang terus-menerus dan tidak kunjung hilang, memiliki faktor risiko seperti merokok dan konsumsi alkohol, atau bahkan kelebihan berat badan dan berada di usia lima puluhan, jangan ragu untuk berkonsultasi dengan dokter umum, dokter spesialis, atau ahli gastroenterologi Anda.




.webp?sfvrsn=20763f7d_21)
.webp?sfvrsn=f2a2c343_12)
 +604–643 8799
+604–643 8799
 Minta Janji Temu
Minta Janji Temu.webp?sfvrsn=276ce14_1/vector-(3).webp) Pasien Internasional
Pasien Internasional.webp)