.webp)
Batu pundi hempedu, atau batu hempedu, merupakan masalah kesihatan yang biasa dan menjejaskan berjuta-juta orang di seluruh dunia. Kelaziman mereka berbeza mengikut kawasan, umur, jantina dan faktor gaya hidup, namun ia merupakan antara gangguan sistem pencernaan yang paling kerap berlaku. Dianggarkan kira-kira 10–15% orang dewasa di negara maju mempunyai batu hempedu, walaupun ramai yang tidak menunjukkan sebarang gejala dan tidak menyedarinya. Batu hempedu lebih kerap berlaku dalam kalangan individu berusia lebih 40 tahun, dengan risikonya meningkat seiring pertambahan usia. Ramai individu yang mempunyai batu hempedu tidak pernah mengalami sebarang gejala; keadaan ini dikenali sebagai “batu hempedu senyap” dan selalunya dikesan secara tidak sengaja semasa imbasan abdomen untuk keadaan lain yang tidak berkaitan. Hanya kira-kira 20–30% daripada individu yang mempunyai batu hempedu akan mengalami gejala atau komplikasi sepanjang hayat mereka.
Catherine, seorang pelajar universiti berusia 23 tahun, hadir ke klinik saya dengan sejarah sakit perut selama tiga tahun yang agak bertambah teruk sejak dua minggu lalu. Dia menggambarkan ketidakselesaan berterusan di bahagian atas perut yang tercetus selepas mengambil makanan pedas dan sejak itu mengelakkan hidangan sebegitu. Kadang-kadang, apabila kesakitan menjadi terlalu lama dan tidak tertanggung, dia mengambil ubat yang dijual di kaunter untuk melegakan gejalanya. Ubat-ubatan ini termasuk alginat (Gaviscon dan Alucid), antasid (Cimetidine), dan perencat pam proton (PPI) seperti Omeprazole dan Pantoprazole. Beberapa hari sebelum hadir ke klinik, kesakitannya bertambah teruk selepas makan malam. Rakan sekelasnya, yang juga mengalami masalah gastrik, berkongsi beberapa ubat dengannya — yang kemudian dikenal pasti sebagai penyekat asid kompetitif kalium (Vocinti). Ubat ini memberikan kelegaan, walaupun tidak serta-merta; ia mengambil masa kira-kira satu jam sebelum dia berasa selesa.
Keesokan harinya, kesakitannya kembali, dan walaupun kurang teruk berbanding hari sebelumnya, dia memutuskan untuk membuat janji temu untuk berjumpa saya dan dimasukkan ke hospital bagi pengurusan kesakitan serta penilaian lanjut. Pemeriksaan awal, termasuk ujian darah menyeluruh, biasa-biasa sahaja, dan imbasan ultrabunyi abdomen mendedahkan batu hempedu. Apabila diperiksa dengan lebih teliti, tiada bukti keradangan pada pundi hempedu. Dia memilih untuk tidak menunggu ujian nafas urea bagi menolak jangkitan Helicobacter pylori, yang juga boleh menyebabkan gejala serupa, kerana dia merasakan dia tidak boleh menghentikan ubat penyekat asidnya untuk jangka masa yang cukup bagi memenuhi syarat penilaian tidak invasif itu. Oleh itu, dia menjalani endoskopi saluran gastrousus atas, yang menunjukkan keadaan biasa-biasa sahaja. Dia discaj tiga hari kemudian dengan diagnosis kemungkinan kolik biliari, dan diberikan preskripsi beberapa PPI, analgesik, parasetamol, serta agen antispasmodik. Dia juga diberi penerangan mengenai dispepsia fungsional dan dimaklumkan tentang pencetus yang berpotensi seperti makanan dan tekanan.
Tiga hari selepas discaj, dia kembali pada waktu malam dengan sakit perut yang teruk selepas makan malam. Disebabkan kesakitan yang teruk, dia dimasukkan semula ke hospital untuk pengurusan kesakitan. Dia telah makan hidangan hot pot bersama keluarganya, dan walaupun semua orang lain baik-baik sahaja, dia pula tidak. Kali ini, selain kesakitan perut, dia juga mengalami demam ringan, loya, muntah berulang, dan najis cair. Ujian fungsi hatinya menunjukkan keabnormalan yang ketara, dengan semua parameter hatinya meningkat lebih daripada 5–7 kali ganda daripada had atas yang normal. Diagnosis keradangan pundi hempedu (kolesistitis) dan batu saluran hempedu (koledokolitiasis) disyaki dan kemudian disahkan melalui imbasan CT abdomen. Dia menjalani prosedur endoskopi untuk membuang batu tersebut dan dimasukkan ke hospital selama beberapa hari untuk menerima antibiotik secara intravena. Pilihan untuk pembuangan pundi hempedu dibincangkan, kerana masih terdapat banyak batu kecil di dalam pundi hempedu, bagi mencegah episod komplikasi berkaitan batu pada masa hadapan. Walaupun dia mengambil masa untuk membuat keputusan, akhirnya keluarga dan pesakit bersetuju untuk meneruskan pembedahan bagi membuang pundi hempedunya (kolesistektomi). Dia discaj dalam keadaan sihat dan kekal sihat sepanjang tempoh susulan sehingga dia sepenuhnya discaj dari jagaan saya.
Hock Soon, seorang lelaki berusia 44 tahun dengan sejarah diabetes dan hipertensi kronik, dimasukkan ke hospital selepas mengalami seminggu sakit perut yang teruk, loya, muntah, lesu, cirit-birit, dan demam ringan. Tekanan darahnya sangat rendah pada 80/40 mmHg, kadar degupan jantungnya tinggi pada 160 bpm, dan tahap oksigen dalam darahnya hanya 88% walaupun menerima oksigen tambahan. Dia dipindahkan ke ICU, diberikan alat oksigen tidak invasif yang lebih kuat, dan disokong dengan tiga ubat inotropik untuk menstabilkan tekanan darahnya. Diagnosis awal mencadangkan ketoasidosis diabetes, dengan paras gula darah yang tinggi (30 mmol/L) dan keton darah yang tinggi (4.3 mmol/L). Rawatan dimulakan serta-merta tanpa menunggu keputusan makmal. Apabila keputusan tiba, ujian fungsi hati dan penanda keradangannya didapati sangat abnormal. Imbasan CT abdomen menunjukkan batu pundi hempedu bersaiz besar 2 cm dan batu bersaiz serupa 2.5 cm di dalam saluran hempedu biasa tengah. Biasanya, saluran hempedu biasa bersaiz kurang daripada 6–8 mm, jadi batu bersaiz 25 mm adalah sangat besar dan seterusnya memburukkan punca penyakitnya. Saluran hempedu di atas batu tersebut bengkak akibat aliran hempedu tersumbat, mengakibatkan penyakit teruk yang disebabkan oleh stasis hempedu yang dijangkiti. Diagnosis kolangitis sekunder kepada koledokolitiasis mendorong rakan sekerja saya untuk menghubungi saya bagi mendapatkan konsultasi. Dalam beberapa jam, prosedur ERCP kecemasan dijalankan untuk mengurangkan halangan hempedu dengan pemasangan stent, tetapi batu tidak dibuang pada peringkat ini kerana jangkitan yang teruk dan risiko memburukkan sepsisnya.
Ubat antibiotik Hock Soon dinaik taraf kepada jenis yang dapat menembusi sistem hempedu dengan berkesan, berserta rawatan sokongan lain. Dalam beberapa hari berikutnya, dia menunjukkan pemulihan yang luar biasa, dari hampir menemui maut kepada meminta makanan dan minuman kegemarannya dengan gembira. Kemudian, dia dirujuk kepada rakan pakar bedah kami, yang merancang untuk menjalankan pembedahan pundi hempedu elektif, pembuangan batu, dan pembinaan semula saluran hempedu dalam beberapa minggu akan datang. Tiga bulan kemudian, bapa Hock Soon mengunjungi saya di klinik atas sebab yang berbeza; sejak saya discajkan anaknya selepas pasukan pembedahan mengambil alih, saya tidak lagi berjumpa dengannya. Rasa terima kasih yang tulus dari hatinya benar-benar menyentuh saya, kerana Hock Soon adalah anak tunggalnya yang sangat disayanginya. Detik-detik sebegini mengingatkan saya mengapa saya memilih untuk menjadi seorang doktor, dan bagaimana ERCP, apabila dilakukan dengan berhati-hati dan dalam keadaan yang sesuai, boleh mengubah tragedi yang berpotensi menjadi nyawa yang diselamatkan.
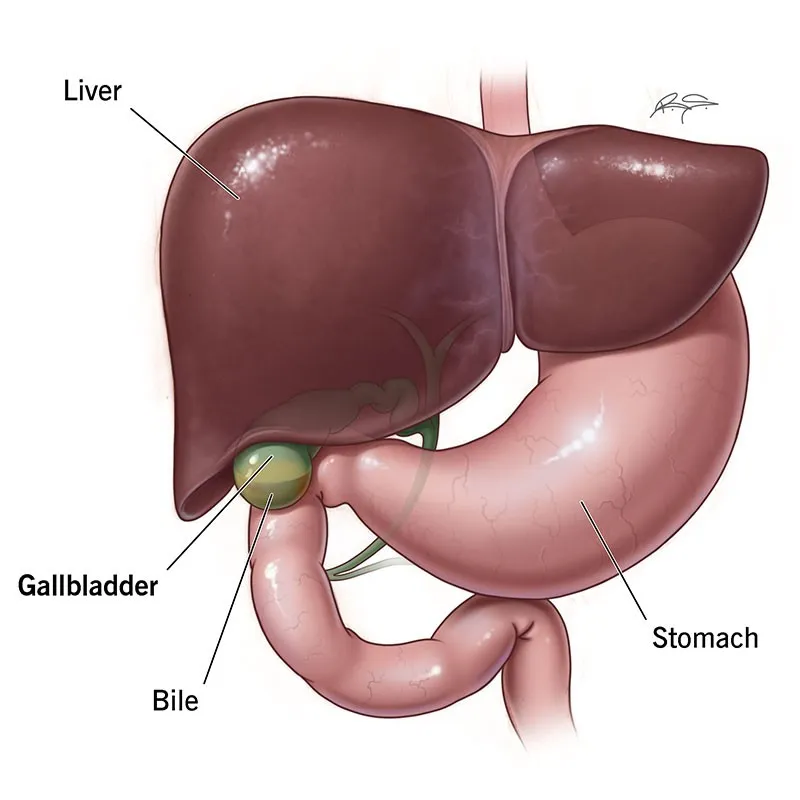
Rajah 1: Lokasi anatomi pundi hempedu (imej dipetik daripada laman web Cleveland Clinic).
Terselip dengan selesa di dalam kawasan hati, tepat di bawah lobus kanan, terdapat sebuah organ kecil berbentuk seperti pir dan berongga yang menjalankan fungsinya dengan senyap tanpa perlu diarahkan. Sering dibincangkan dalam kalangan masyarakat kita kerana kekerapan berlakunya batu pundi hempedu, organ ini biasanya diabaikan sebagai punca utama sakit perut sehingga ujian menunjukkan sebaliknya. Ini kerana perut sering disyaki sebagai punca semua sakit perut, memandangkan kaitannya dengan gejala yang berkaitan dengan pengambilan makanan dan waktu makan.
Perut juga merupakan organ yang lebih dikenali orang ramai, berbanding pundi hempedu yang lebih sukar dijangkau dan kurang difahami. Mungkin orang lebih cenderung menyalahkan perut kerana rawatannya lebih mudah, selalunya hanya memerlukan sebiji pil atau seteguk alginat berperisa susu, berbanding perlu ke hospital untuk ujian darah, imbasan, atau mungkin konsultasi pembedahan. Oleh kerana ubat gastrik juga tersedia secara meluas di farmasi tempatan, andaian orang ramai bahawa semua masalah perut mereka berasal dari perut itu sendiri menjadi sedikit kukuh.
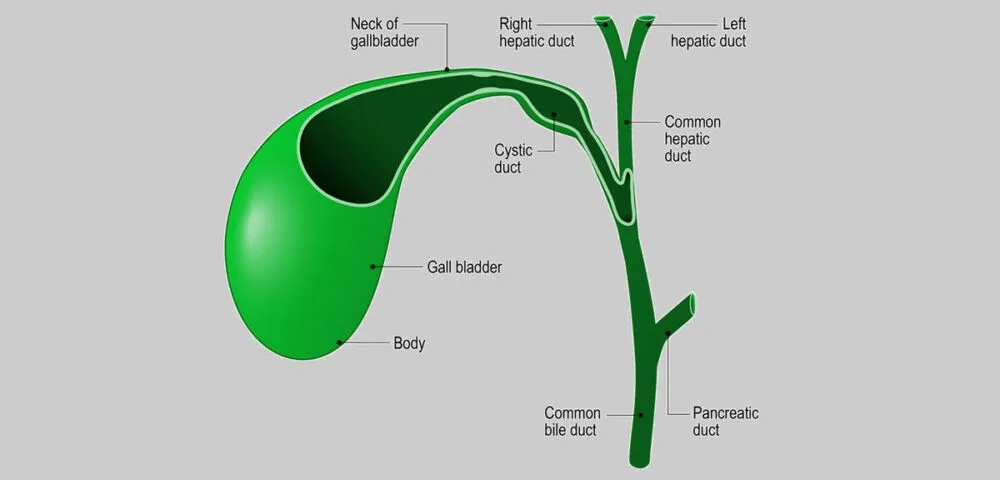
Rajah 2: Struktur pundi hempedu berkaitan dengan saluran kistik, saluran hepatik biasa, saluran hempedu biasa, dan saluran pankreas (imej dipetik daripada laman web Patologi Johns Hopkins).
Sebenarnya, pundi hempedu sama pentingnya, jika tidak, lebih penting. Organ ini biasanya bersaiz 7 hingga 10 cm panjang dan 4 cm lebar pada orang dewasa, dengan kapasiti sekitar 50 mililiter. Pundi hempedu kita berfungsi sebagai takungan simpanan untuk hempedu. Ia menerima hempedu daripada hati, menyimpannya, dan kemudian melepaskan hempedu yang pekat ke dalam usus kecil dalam jumlah terkawal semasa waktu makan untuk membantu pencernaan lemak. Secara normal, pundi hempedu mengecut selepas makan dan mengembang sepenuhnya semasa berpuasa. Inilah sebabnya doktor sering menasihatkan pesakit supaya berpuasa (tidak mengambil apa-apa melalui mulut) sebelum imbasan ultrabunyi abdomen, bagi membolehkan doktor melihat organ tersebut dengan lebih jelas.
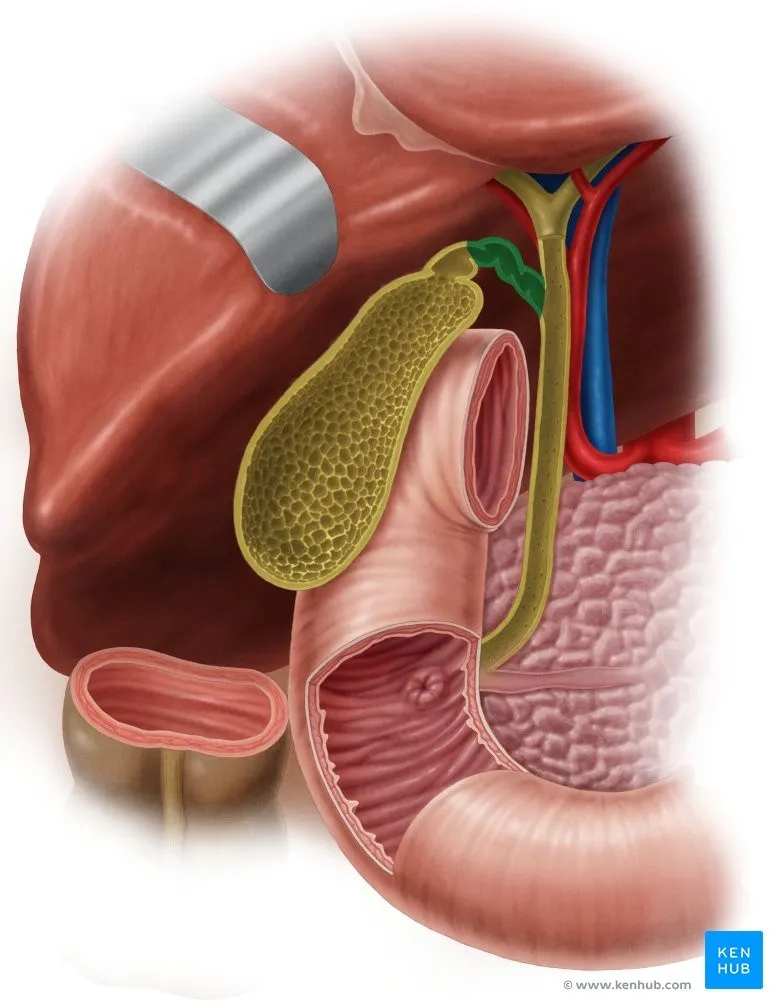
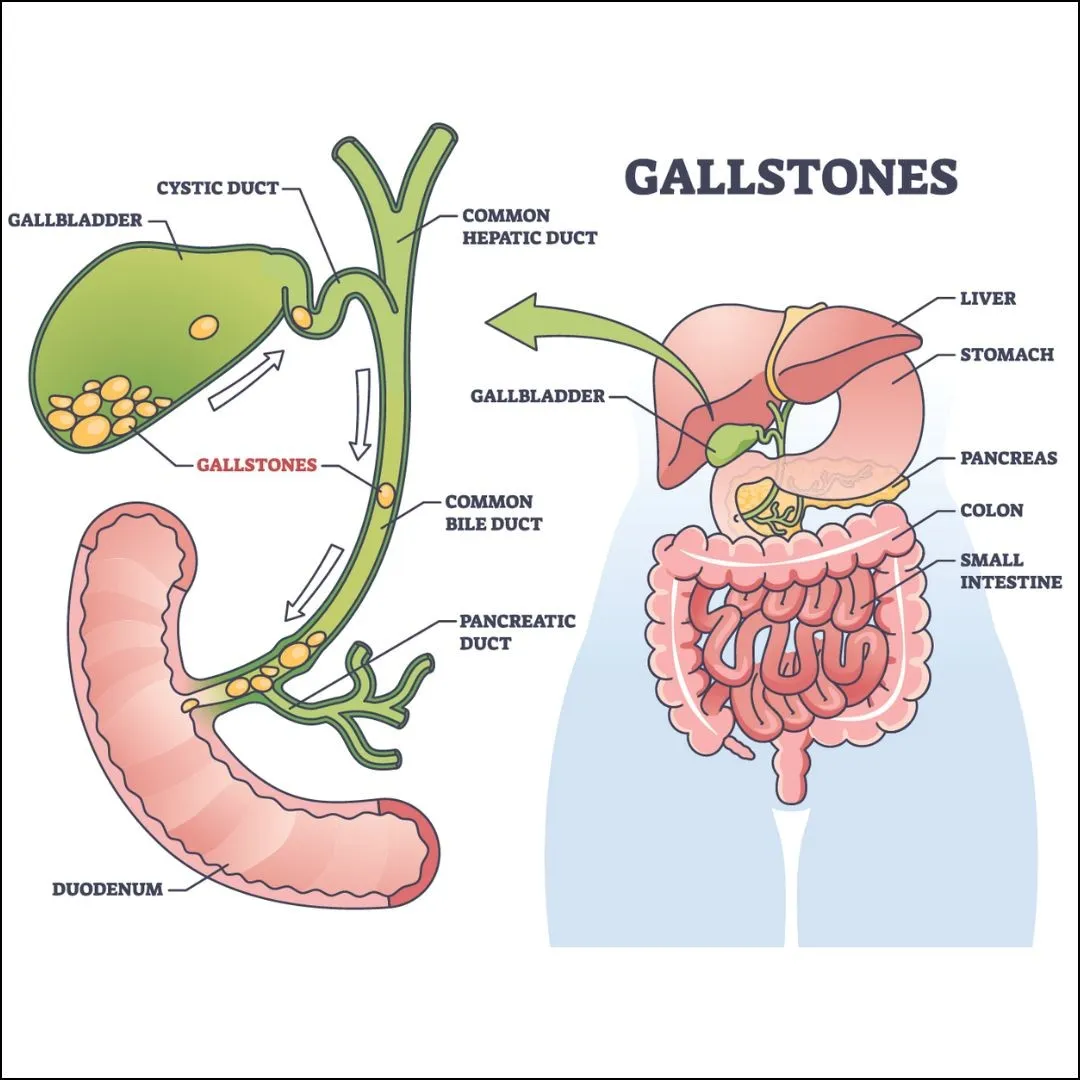
Rajah 3: Imej terurai pundi hempedu yang terletak tepat di bawah lobus kanan hati, di hadapan duodenum (bahagian pertama usus kecil), di atas dan di hadapan usus besar (ditunjukkan di sini sebagai kolon menaik – bahagian kanan bawah imej ini), serta berhampiran kepala pankreas (imej dipetik daripada laman web www.kenhub.com).
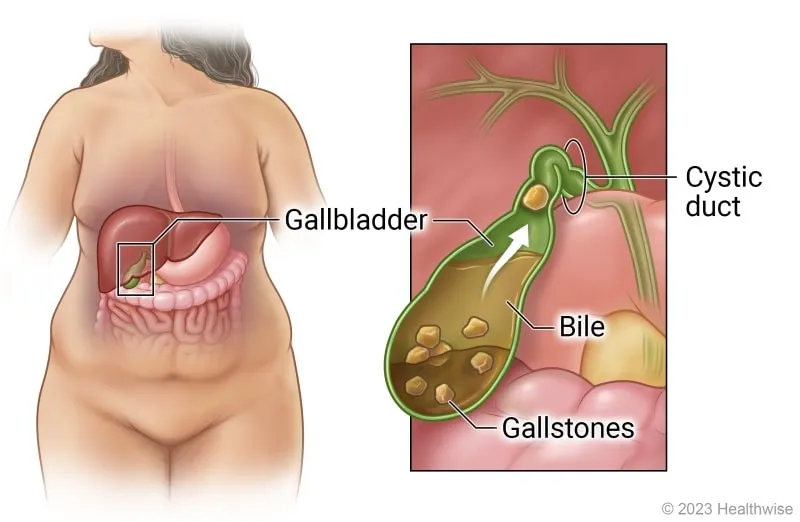
Rajah 4: Ilustrasi kartun yang menunjukkan bagaimana batu hempedu terbentuk di dalam pundi hempedu (imej dipetik daripada laman web UK Health Care).
Batu pundi hempedu mungkin merupakan masalah yang paling kerap menjejaskan pundi hempedu dalam kalangan manusia. Ia terbentuk apabila mendapan hempedu mengeras di dalam pundi hempedu. Kebanyakan masa, ia berada secara senyap di dalam organ tersebut tanpa menyebabkan sebarang gejala atau menunjukkan kewujudannya. Ramai pesakit hidup dengan batu sebegini sepanjang hayat tanpa menyedarinya, dan selalunya hanya mengetahuinya semasa saringan kesihatan tahunan atau pemeriksaan rutin. Pesakit kemudian diyakinkan bahawa tiada sebab untuk bimbang, digalakkan mengekalkan gaya hidup aktif, dan dinasihatkan mengawal pemakanan dengan mengurangkan makanan berminyak, berlemak, ultra-diproses, serta makanan yang diproses. Pemantauan hanya diperlukan sekiranya gejala baharu muncul.

Rajah 5: Batu hempedu seperti yang kelihatan di luar tubuh manusia (imej dipetik daripada laman web Pace Hospitals).
Sebaliknya, sesetengah pesakit menemui batu hempedu mereka dalam keadaan yang kurang menguntungkan, seperti yang berlaku pada pesakit kami, Hock Soon. Gejala yang paling biasa termasuk sakit perut yang samar, episodik, biasanya berlangsung beberapa jam, dan kemudian hilang secara tiba-tiba. Semasa episod ketidakselesaan sebegini, seseorang yang waras biasanya akan mencuba ubat yang dijual di kaunter seperti alginat, antasid, dan bahkan ubat ‘gastrik’ yang lebih kuat. Kadang-kadang, gejala itu akan hilang dengan sendirinya, tetapi jika kesakitan meningkat, pesakit tiada pilihan selain mendapatkan nasihat daripada doktor perubatan am mereka. Berdasarkan keadaan dan penemuan awal, doktor perubatan am mungkin akan mengarahkan ujian makmal tambahan dan imbasan ultrabunyi jika kemudahan tersebut tersedia. Jika tidak, mereka akan merujuk pesakit kepada pakar di hospital untuk konsultasi lanjut.
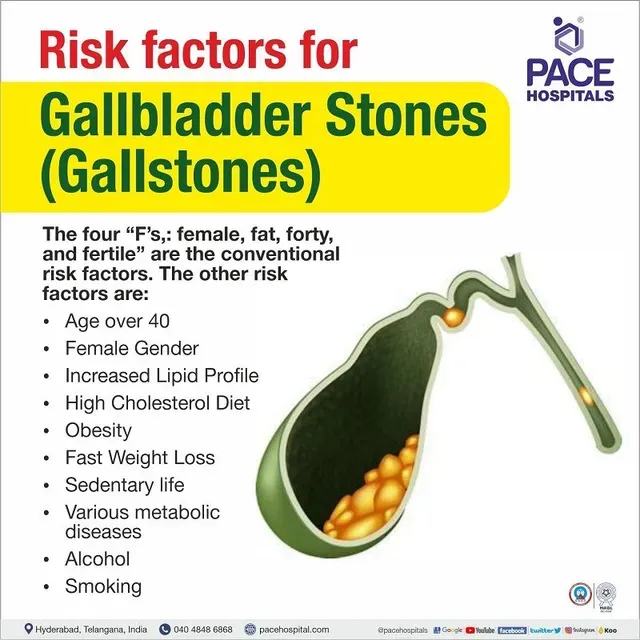
Rajah 6: Ringkasan faktor risiko pembentukan batu pundi hempedu, menunjukkan empat 'F' tradisional seperti yang digambarkan dalam kartun ini (imej dipetik daripada laman web PACE Hospitals).
Batu pundi hempedu, bergantung pada lokasinya di luar pundi hempedu, boleh menyebabkan pelbagai jenis sakit, berbeza dari segi keterukan dan gejala yang berkaitan. Adalah berguna untuk memahami beberapa istilah utama yang berkaitan dengan bagaimana batu pundi hempedu boleh menyebabkan pelbagai ketidakselesaan.
Rajah 7: Perwakilan bergambar bagi pelbagai lokasi batu pundi hempedu dan masalah yang timbul – batu yang tersangkut di dalam saluran sistik menyebabkan kolesistitis, manakala batu yang tersangkut di dalam saluran hempedu biasa dikenali sebagai koledokolitiasis (imej dipetik daripada laman web Continental Hospital).
Kolik hempedu berlaku apabila batu tersangkut di dalam saluran sistik, yang merupakan saluran keluar dari pundi hempedu. Sering dirujuk sebagai serangan pundi hempedu atau serangan batu pundi hempedu, sakit ini digambarkan sebagai kolik—datang dan pergi secara beralun disebabkan pengecutan otot organ berongga. Ini berlaku apabila pundi hempedu cuba menolak hempedu melepasi batu tersebut. Rasa sakit biasanya terletak di bahagian atas kanan abdomen dan berlangsung antara 15 minit hingga beberapa jam. Pesakit sering melaporkan bahawa mereka baru sahaja mengambil makanan yang berat dan berlemak sebelum itu. Jika ia berlaku selepas makan malam, pesakit mungkin sukar tidur, menyebabkan sesetengahnya mendapatkan rawatan di jabatan kecemasan atau klinik pada waktu malam, kerana bimbang mereka mengalami sakit ‘gastrik’ yang teruk atau serangan jantung. Biasanya, pesakit kami menerima analgesik secara intramuskular atau intravena, penghambat pam proton, dan ubat simptomatik lain. Selepas berehat seketika, mereka selalunya berasa cukup sihat untuk discaj dalam masa satu atau dua jam. Kebanyakan pesakit tidak kembali untuk susulan dan meneruskan aktiviti harian seperti biasa sehingga serangan kedua atau seterusnya berlaku.
Gejala biasa termasuk sakit yang tajam, kekejangan, atau tumpul dengan tahap keterukan yang berbeza-beza. Sakit itu mungkin merebak ke hujung bahu kanan atau ke dada (yang boleh meniru serangan jantung). Pesakit juga mengadu rasa loya, muntah, selera makan berkurangan, dan masalah pencernaan. Kesakitan hilang serta-merta apabila batu sama ada terus kembali ke dalam pundi hempedu atau bertambah kuat jika ia bergerak ke bawah ke saluran hempedu biasa.
Kolesistitis berlaku apabila batu hempedu tersangkut atau tersekat di dalam saluran sistik dan tidak bergerak. Ia tidak dapat kembali ke pundi hempedu atau melepasi saluran hempedu biasa. Akibatnya, hempedu tidak dapat mengalir keluar ke dalam usus kecil dan mula terkumpul di dalam pundi hempedu. Ini menyebabkan pundi hempedu membengkak, meregangkan permukaan organ dan merengsakan reseptor sakit, yang membawa kepada kesakitan yang kuat dan berterusan. Kolik hempedu kemudiannya berkembang menjadi kolesistitis akut, di mana keradangan berlaku. Bersama simptom kolik hempedu, pesakit kini mengalami demam akibat jangkitan. Satu gejala tambahan, jaundis—penguningan kulit—juga boleh muncul jika keradangan pundi hempedu menceroboh hati yang berdekatan atau jika bengkak saluran sistik menjejaskan saluran hempedu biasa (sindrom Mirizzi).
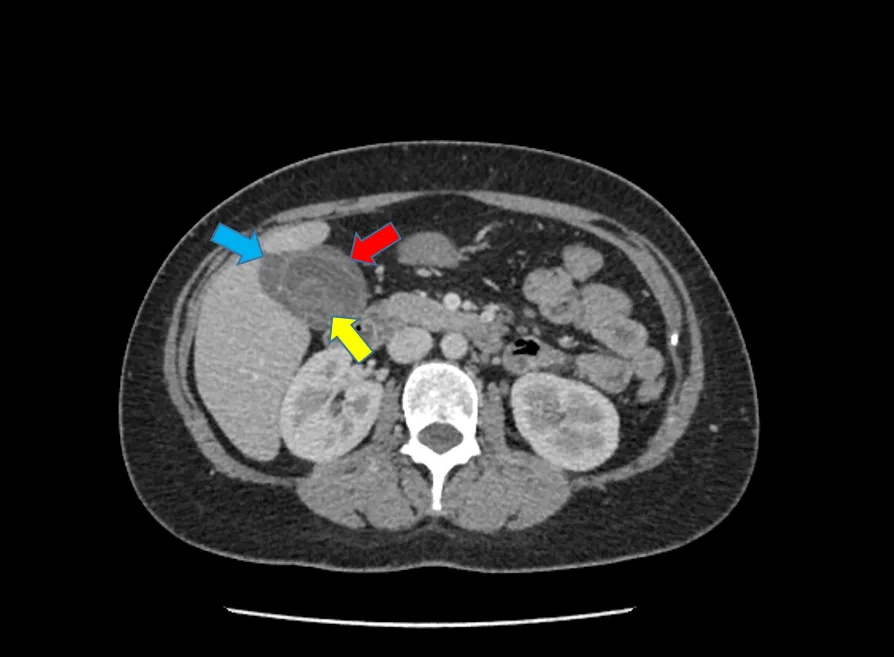
Rajah 8: Cholelithiasis (batu pundi hempedu – panah kuning) dan cholecystitis (radang pundi hempedu yang ditunjukkan oleh dinding pundi hempedu yang menebal – panah merah, dan cecair radang di sekeliling pundi hempedu – panah biru).
Keadaan kolesistitis akut memerlukan perhatian perubatan segera dan selalunya memerlukan kemasukan ke hospital untuk rawatan antibiotik intravena, ubat anti-radang, bendalir untuk memulihkan dehidrasi, dan ubat-ubatan simptomatik untuk loya dan muntah. Ujian darah berguna untuk menilai tahap keterukan keabnormalan fungsi hati, keputusan panel jangkitan, dan kultur darah, yang menjadi panduan dalam pemilihan antibiotik. Pesakit harus menjangkakan prosedur pengimejan, seperti ultrabunyi dan/atau imbasan CT, sebagai asas untuk mengesahkan diagnosis serta menilai tahap keterukan dan komplikasi kolesistitis akut. Ujian-ujian ini memberikan maklumat klinikal dan diagnostik yang menyeluruh untuk membantu doktor memahami keadaan anda dengan lebih baik serta berbincang dengan anda mengenai kemungkinan keperluan pembedahan dan waktunya, sekiranya perlu.
Choledocholithiasis dan kolangitis – istilah 'choledocholithiasis' merujuk kepada keadaan di mana batu hempedu bergerak lebih jauh ke dalam saluran sistik dan jatuh ke dalam saluran hempedu biasa, tersangkut di hujung saluran tersebut dan menyebabkan penyumbatan aliran hempedu. Keadaan sebegini menyebabkan hempedu tersekat, yang seterusnya menggalakkan jangkitan dan, dari masa ke masa, menyebabkan pembengkakan saluran hempedu serta aliran hempedu balik ke dalam hati. Tanpa rawatan segera, pesakit berisiko mengalami kolangitis – keradangan pada saluran hempedu – dan, dalam kes yang teruk, septikemia, iaitu apabila jangkitan merebak ke dalam aliran darah, yang berpotensi mengancam nyawa. Kemasukan ke hospital menjadi perlu bukan sahaja untuk memulakan langkah-langkah menyelamatkan nyawa bagi keadaan seperti kolesistitis akut, tetapi juga untuk membolehkan prosedur tepat pada masanya bagi mengurangkan tekanan pada saluran hempedu dengan meletakkan tiub plastik untuk memulihkan aliran hempedu. Pemasangan stent ini dilakukan melalui prosedur endoskopik yang dipanggil endoskopik retrograd kolangiopankreatografi (atau ERCP).
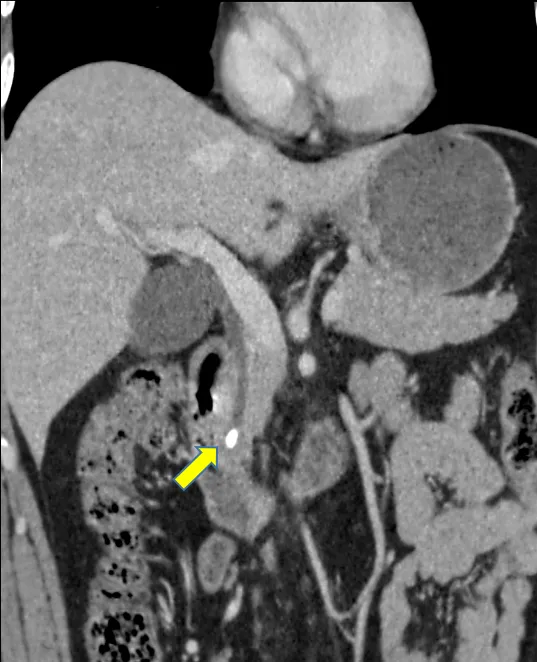
Rajah 9: Choledocholithiasis (batu hempedu dalam saluran hempedu biasa – anak panah kuning).
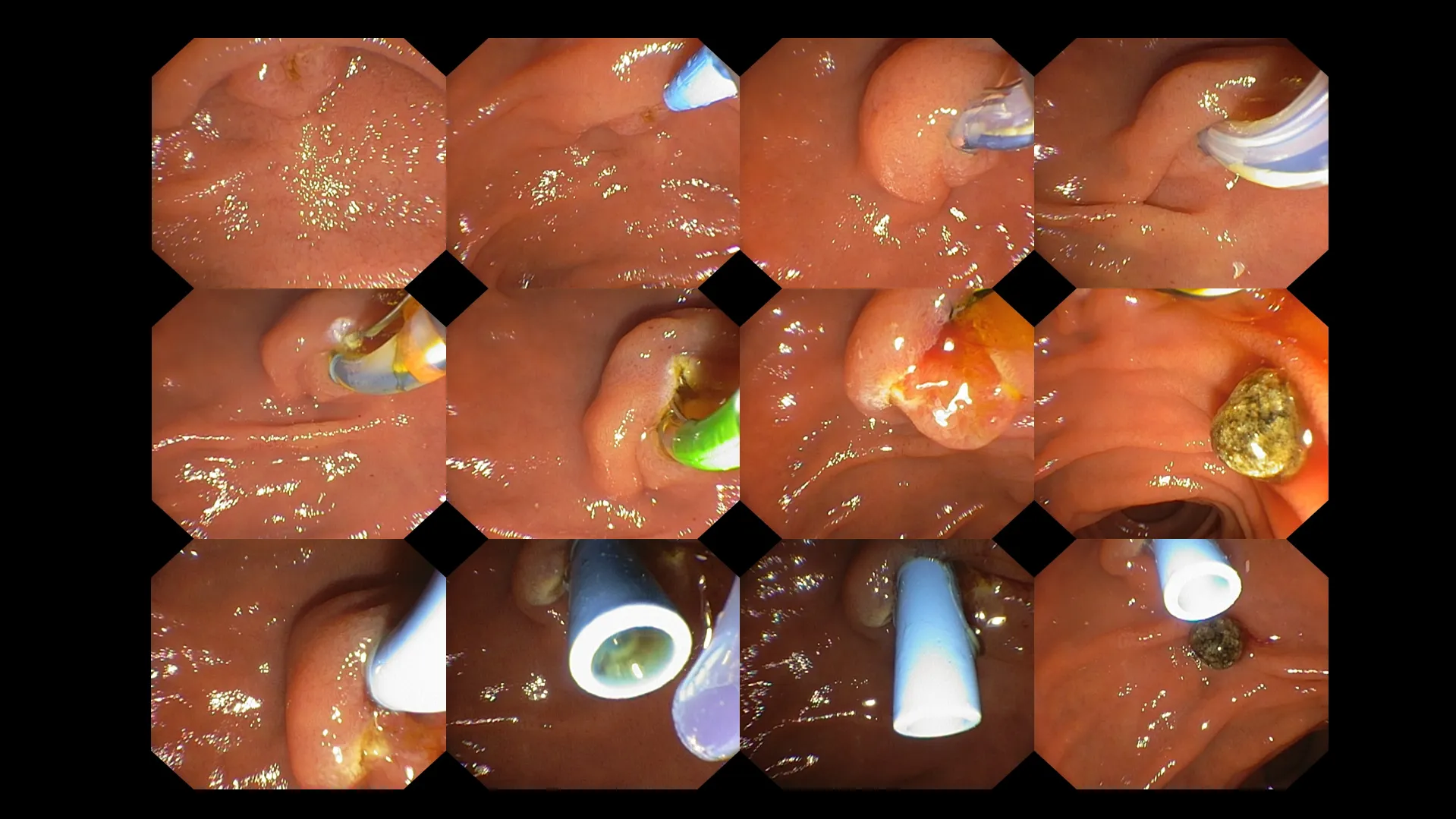
Rajah 10: Endoskopik retrograd kolangiopankreatografi (ERCP) dijalankan ke atas pesakit yang mempunyai batu hempedu tersangkut dalam saluran hempedu biasa (choledocholithiasis). Pendekatan langkah demi langkah digunakan untuk mengenal pasti pintu masuk ke dalam saluran hempedu biasa, diikuti dengan pemasangan kateter yang dilengkapi dengan wayar panduan ke dalam laluan hempedu. Pintu masuk (ampula) kemudian dipotong sedikit untuk membolehkan pengeluaran batu. Selepas pengeluaran batu berjaya, sebuah stent sementara (tiub biru, dilihat pada baris terakhir imej di atas) dipasang untuk mengurangkan tekanan pada saluran hempedu, membolehkan aliran hempedu bergerak dengan bebas.
Pesakit dengan kolangitis biasanya tinggal di hospital selama beberapa hari untuk memantau tindak balas mereka terhadap antibiotik, menunggu keputusan akhir kultur darah atau hempedu bagi rawatan antibiotik yang khusus, menjalankan ujian makmal secara bersiri untuk menilai tindak balas klinikal dan biokimia keseluruhan, serta memantau kemungkinan komplikasi selepas prosedur ERCP. Tempoh tinggal di hospital ditentukan berdasarkan setiap kes, bergantung kepada keterukan keadaan pesakit.
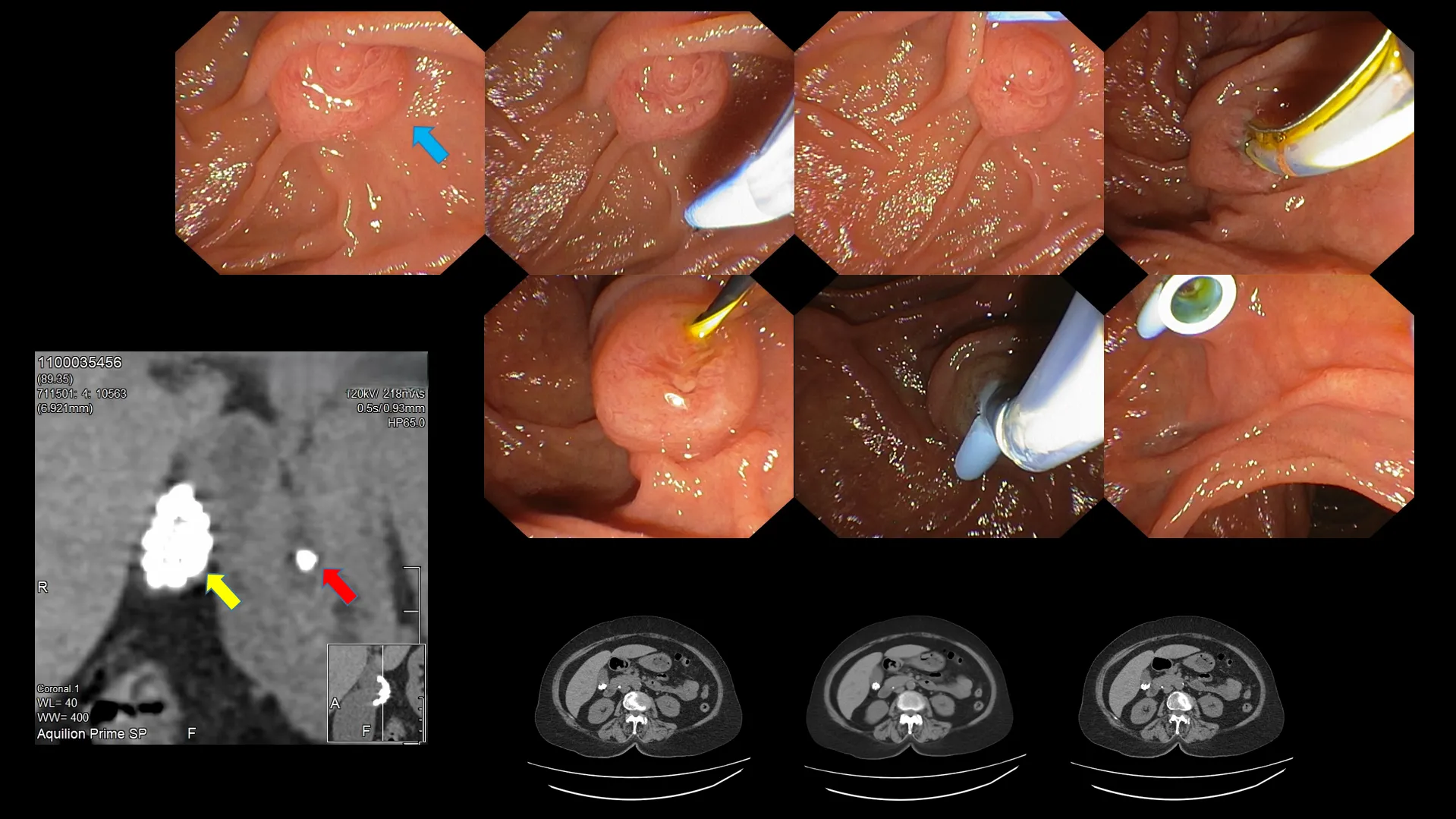
Rajah 11: Contoh lain dengan imej imbasan CT yang disertakan. Batu pundi hempedu (anak panah kuning) dan batu tersangkut dalam saluran hempedu biasa (anak panah merah) dapat dilihat pada imbasan CT. Imej endoskopik ampula (anak panah biru). Pengenalpastian langkah demi langkah pintu masuk ampula, kanulasi dengan wayar panduan, dan pemasangan stent untuk memudahkan aliran hempedu.
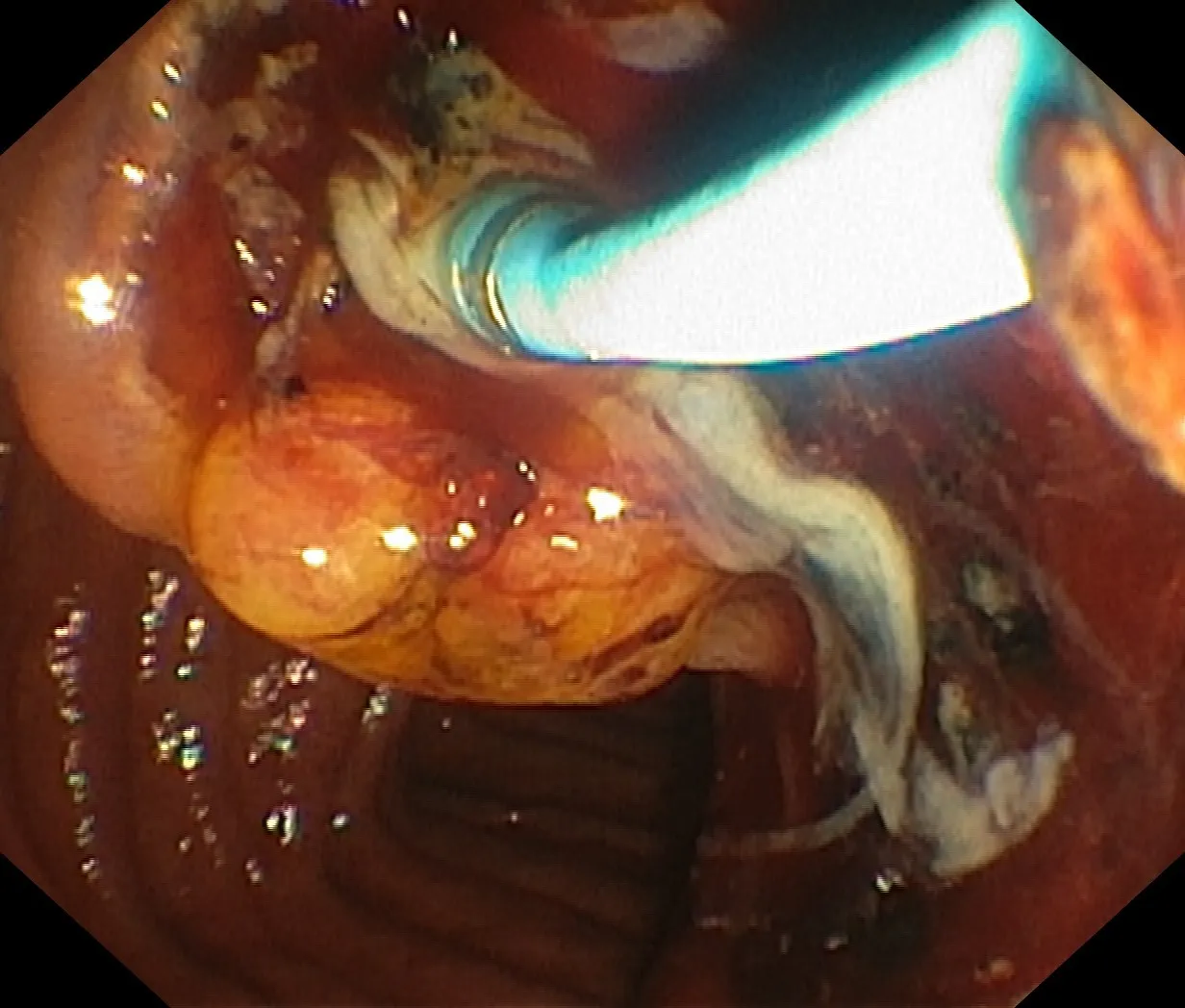
Rajah 12: Kolangitis supuratif (bernanah) sekunder kepada saluran hempedu tersumbat – jejak cecair berwarna putih keruh ialah nanah yang terhasil daripada jangkitan bakteria akibat penyumbatan batu yang berpanjangan di saluran hempedu biasa. Aliran nanah yang banyak berlaku secara tiba-tiba selepas kanulasi ampula berjaya.
Kebimbangan seterusnya adalah tidak dapat dielakkan. Pesakit yang mendapat maklumat secukupnya biasanya tahu apa yang perlu dijangka seterusnya. Doktor mungkin telah berjaya merawat keadaan akut dengan memberikan ubat penahan sakit untuk kolik hempedu, antibiotik untuk kolesistitis akut, menjalankan ERCP dengan pengeluaran batu dan pemasangan stent untuk choledocholithiasis, serta menetapkan antibiotik untuk kolangitis akut, tetapi adakah itu sahaja? Soalan yang berterusan ialah sama ada pembedahan benar-benar diperlukan. Adakah pembuangan pundi hempedu (kolesistektomi) melalui pembedahan terbuka, laparoskopik (lubang kunci), atau kini melalui pembedahan berpandu robot, diperlukan? Daripada menumpukan sepenuhnya pada teknik, isu utama ialah sama ada prosedur itu wajar dilakukan langsung. Ini adalah topik yang kompleks, dan tidak semua orang akan mengalami hasil yang sama. Senario yang jelas yang membawa kepada pembedahan melibatkan pesakit yang, walaupun selepas semua perkara di atas, terus mengalami perkara berikut:-
Rajah 13: Walaupun batu saluran hempedu boleh menyumbat saluran hempedu biasa, ia juga boleh menyebabkan penyumbatan saluran pankreas sama ada secara langsung melalui halangan pada saluran atau secara tidak langsung melalui tindak balas keradangan – bengkak tisu yang menyebabkan tekanan luaran ke atas saluran pankreas. Komik ini menunjukkan bagaimana pundi hempedu membuang batunya ke dalam saluran hempedu, mengakibatkan penyumbatan saluran pankreas dan seterusnya pankreatitis yang disebabkan oleh enzim pankreas yang bersifat korosif (imej dipetik daripada laman web AwkwardYeti.com).
Idea pembedahan sering membimbangkan pesakit kerana tiada siapa yang gembira dengan fikiran untuk menjalani pembedahan. Doktor anda akan dapat menerangkan pelbagai sebab yang mungkin memerlukan kolesistektomi, masa yang sesuai untuk prosedur tersebut, komplikasi yang mungkin timbul bergantung pada teknik yang digunakan, serta apa yang boleh dijangkakan selepas pembedahan.
Saya kerap menerima soalan tentang sama ada seseorang boleh hidup tanpa pundi hempedu mereka. Seperti apendiks, pembuangannya tidak menjejaskan kehidupan normal dan sihat pesakit. Hati akan terus menghasilkan hempedu, jadi anda masih boleh mencerna lemak daripada makanan berlemak.
Perbezaan satu-satunya sekarang ialah anda tidak lagi mempunyai pundi hempedu untuk menyimpan dan memekatkan hempedu anda. Anda juga kehilangan keupayaan untuk mengawal jumlah rembesan cecair hempedu mengikut jenis makanan yang diambil. Sebaliknya, hempedu daripada hati mengalir terus ke usus kecil, bukannya dirembeskan secara tersasar atau berkala. Akibatnya, sesetengah pesakit mungkin mengalami cirit-birit serta pengeluaran gas atau kembung yang berlebihan selepas mengambil makanan berlemak. Cirit-birit berlaku kerana hempedu yang berterusan dan kurang pekat boleh merengsakan usus dan bertindak seperti julap, menyebabkan cirit-birit asid hempedu. Kembung berlaku disebabkan penghadaman lemak yang terganggu, yang juga berpunca daripada prinsip yang sama iaitu hempedu yang kurang pekat.
Rajah 14: Fungsi utama pundi hempedu seperti yang diterangkan oleh aktiviti ektrakurikulum bagi hati dan pundi hempedu (imej dipetik daripada laman web AwkwardYeti.com)
Jadi, pundi hempedu saya telah dibuang. Apakah seterusnya? Bagaimana saya boleh memastikan keadaan saya berada pada tahap optimum?
Daripada mengambil hidangan besar seperti biasa, pilih hidangan yang lebih kecil tetapi lebih kerap. Ini membantu sistem pencernaan anda memproses lemak dan nutrien dengan lebih berkesan, sekaligus mengurangkan risiko kembung dan ketidakselesaan.
Ramai yang percaya bahawa anda mesti mengelakkan lemak sepenuhnya, tetapi itu adalah salah faham. Tubuh masih memerlukan lemak sihat untuk tenaga, fungsi sel, dan penyerapan vitamin. Walau bagaimanapun, kerana hempedu tidak lagi dilepaskan secara pekat dan terkawal, adalah wajar untuk:
Sesetengah individu mendapati bahawa sesetengah makanan—terutamanya yang tinggi lemak atau pedas—boleh menyebabkan ketidakselesaan atau cirit-birit selepas pembedahan. Perkenalkan makanan ini secara berperingkat untuk menilai toleransi peribadi anda. Setiap orang berbeza, dengan had toleransi masing-masing. Jangan takut untuk bereksperimen dengan pelbagai jenis makanan bagi melihat bagaimana tubuh anda bertindak balas.
Menambahkan pengambilan serat larut secara berperingkat (ditemui dalam oat, epal, lobak, dan kacang) dapat membantu menormalkan pergerakan usus dan mencegah cirit-birit. Walau bagaimanapun, peningkatan serat terlalu cepat boleh menyebabkan angin atau kembung, jadi adalah lebih baik diperkenalkan secara berperingkat.
Minum air yang mencukupi menyokong pencernaan dan membantu mencegah sembelit, yang kadangkala berlaku selepas pembedahan..
Sesetengah orang mengalami intoleransi laktosa sementara selepas pembedahan pundi hempedu. Jika anda mengalami ketidakselesaan pencernaan dengan produk tenusu, cuba pilihan bebas laktosa atau kurangkan pengambilan sehingga sistem anda menyesuaikan diri.
Kebanyakan orang akhirnya boleh menikmati jumlah lemak yang sederhana. Mulakan secara perlahan dan perhatikan bagaimana tubuh anda bertindak balas.
Biasanya, suplemen enzim tidak diperlukan. Tubuh anda biasanya menyesuaikan diri, tetapi jika anda mengalami kesukaran yang berterusan, doktor anda mungkin mencadangkan rawatan tertentu.
Ya, namun, seperti mana-mana pembedahan, berbincanglah rancangan anda dengan penyedia penjagaan kesihatan untuk memastikan hasil yang terbaik.
Tiada makanan yang benar-benar dilarang, tetapi bersederhana adalah kunci. Fokus pada diet seimbang, yang kaya dengan nutrien.
Hidup tanpa pundi hempedu adalah sepenuhnya mungkin, dan kebanyakan orang mendapati mereka boleh kembali kepada diet dan gaya hidup normal dalam beberapa bulan selepas pembedahan. Walaupun beberapa penyesuaian sementara terhadap tabiat pemakanan mungkin diperlukan, tubuh anda sangat mudah menyesuaikan diri. Menekankan hidangan kecil, lemak sihat, dan serat, sambil mendengar isyarat tubuh, dapat membantu anda menikmati kehidupan sepenuhnya. Jika anda mengalami gejala yang berterusan atau teruk, dapatkan nasihat daripada penyedia penjagaan kesihatan untuk panduan dan sokongan.




.webp?sfvrsn=20763f7d_21)
.webp?sfvrsn=f2a2c343_12)
 +604–643 8799
+604–643 8799
 Minta temu janji
Minta temu janji.webp?sfvrsn=276ce14_1/vector-(3).webp) Pesakit Antarabangsa
Pesakit Antarabangsa.webp)