.webp)

Saya rasa kembung, doktor. Perut saya rasa seperti dram.
Ini merupakan kenyataan paling lazim yang saya dengar hampir setiap hari sebagai seorang pakar gastroenterologi yang berkhidmat di sebuah hospital swasta di Pulau Pinang. Malah, semasa perbualan santai bersama rakan dan ahli keluarga pada hari cuti, mereka sering berkongsi keluhan berkaitan sistem penghadaman mereka. Kebiasaannya, saya dapat meneka bahawa aduan tersebut berkisar pada salah satu daripada tiga perkara: sakit perut, perut kembung, atau pedih ulu hati yang berpanjangan. Walaupun saya menikmati perbualan santai sebegini, perbincangan sering kali berubah menjadi sesuatu yang lebih serius.
Dari sudut perubatan, kembung merujuk kepada sensasi subjektif rasa perut mengembang, membengkak, atau penuh, yang dialami apabila dinding abdomen menjadi tegang dan kadangkala terasa keras. Keadaan ini lazimnya tidak menyebabkan kesakitan teruk sehingga memerlukan rawatan kecemasan, namun ketidakselesaannya sering mendorong pesakit mendapatkan nasihat perubatan. Keadaan ini menjejaskan kualiti hidup pesakit, kerana mereka tidak dapat menikmati hidangan sepenuhnya, sering berasa loya, dan dalam sesetengah keadaan, mengalami muntah. Apabila berlaku pada waktu malam, keadaan ini boleh mengganggu tidur akibat rasa berat di perut. Perut kembung boleh berpunca daripada lebihan gas, cecair, najis, ketumbuhan pepejal, atau malah kehamilan yang belum dikenal pasti. Keadaan ini menjadi lebih mengelirukan apabila pesakit daripada pelbagai peringkat umur, etnik, jantina, dan bentuk badan hadir mendapatkan rawatan bagi masalah 'kembung' yang sama.

Rajah 1: Kembung ialah aduan subjektif yang memerlukan penilaian perubatan lanjut sekiranya gejala menjadi berterusan dan mengganggu (imej ihsan Alpine Surgical).
Walaupun keadaan ini kadangkala boleh mengelirukan, proses membantu pesakit merungkai rangkaian gejala yang kompleks dan seterusnya menyediakan penyelesaian yang tepat merupakan sesuatu yang sangat menarik. Ia menjadi lebih bermakna apabila pesakit kembali dan memaklumkan bahawa masalah kembung yang mengganggu mereka selama berminggu-minggu, berbulan-bulan, bertahun-tahun, malah berdekad-dekad, kini telah berlalu. Walaupun saya ingin memberi tumpuan kepada 'kembung berkaitan gastroenterologi', iaitu kembung yang berpunca sepenuhnya daripada gangguan gastroenterologi, hakikatnya keadaan ini tidak selalu demikian. Pesakit kerap mengalami kesukaran dalam membezakan antara gejala dan punca asas yang mendasari keadaan tersebut. Oleh itu, pengamal perubatan perlu sentiasa berwaspada terhadap kemungkinan perangkap dan petunjuk yang mengelirukan ketika mengambil sejarah perubatan terperinci dan pemeriksaan pesakit yang mengadu kembung.
Apakah yang boleh anda jangkakan apabila berkunjung ke klinik untuk masalah kembung? Atau bagaimana anda boleh membuat persediaan sebelum berjumpa pakar gastroenterologi? Saya faham bahawa perasaan cemas terhadap perkara yang tidak diketahui, serta kebimbangan bahawa keputusan yang diterima mungkin tidak menyenangkan, adalah perkara biasa. Terdapat juga kebimbangan terhadap pelbagai ujian yang akan dicadangkan oleh doktor. Penyusunan pemikiran dan aduan utama secara kronologi dapat membantu proses konsultasi, di mana pakar perubatan akan membimbing pesakit menangani kebimbangan yang timbul. Matlamat kami adalah untuk mengenal pasti punca kembung, memahami penyebabnya, dan menyediakan penyelesaian yang sesuai bagi masalah kesihatan anda.
Sedikit perkongsian peribadi…
Sejak memulakan amalan swasta di Pulau Pinang, saya memperoleh banyak pengalaman melalui cabaran dan kerumitan dalam memahami masalah kembung. Saya pernah menemui pelbagai punca kembung yang tidak berkaitan dengan gastroenterologi, termasuk ketumbuhan atau sista ovari bersaiz besar pada remaja perempuan, fibroid rahim yang ketara pada wanita pertengahan usia, batu karang buah pinggang tersangkut pada lelaki obes, kegagalan buah pinggang yang tidak didiagnosis pada warga emas bertubuh kurus, kegagalan jantung dengan diabetes mellitus yang tidak terkawal pada wanita berbadan besar, abses hati pada ahli perniagaan muda yang kerap mengembara, ketumbuhan hati bersaiz besar pada lelaki warga emas, pembesaran limpa akibat gangguan darah pada wanita muda, sista pankreas, gejala perimenopaus, serta tiga kes kehamilan yang tidak didiagnosis dan tidak disangka-sangka.
Diagnosis seperti ini boleh menyerupai kembung yang berpunca daripada masalah gastroenterologi, menyebabkan pesakit mendapatkan kelegaan sementara melalui ubat tanpa preskripsi seperti antasid, alginat (contohnya Gaviscon), dan simetikon (seperti Maalox Plus, Alucid, Gas-X, dan GazGo). Sebaliknya, sesetengah pesakit yang dipengaruhi oleh pengalaman ahli keluarga atau rakan mungkin mencuba ubat tradisional, suplemen, prebiotik, probiotik, serta perencat pam proton (agen peneutral asid) untuk tempoh yang tidak ditentukan tanpa sebarang penambahbaikan. Kelewatan diagnosis akibat pendekatan ini boleh menjadi masalah besar sekiranya punca sebenar akhirnya dikenal pasti sebagai penyakit malignan.
Saya berharap rencana ini dapat membantu meningkatkan kesedaran orang ramai agar mendapatkan nasihat pengamal perubatan am atau rujukan kepada pakar sekiranya terdapat sebarang keraguan atau gejala yang berterusan.
Kini, mari kita beralih kepada isu teras kembung yang berpunca daripada faktor gastroenterologi. Berikut ialah senarai punca yang tersusun dan tidak menyeluruh, namun saya dapati amat berguna dalam suasana klinik yang sibuk. Artikel ini ditulis daripada sudut pandang pengalaman sebenar saya ketika berurusan dengan pesakit:
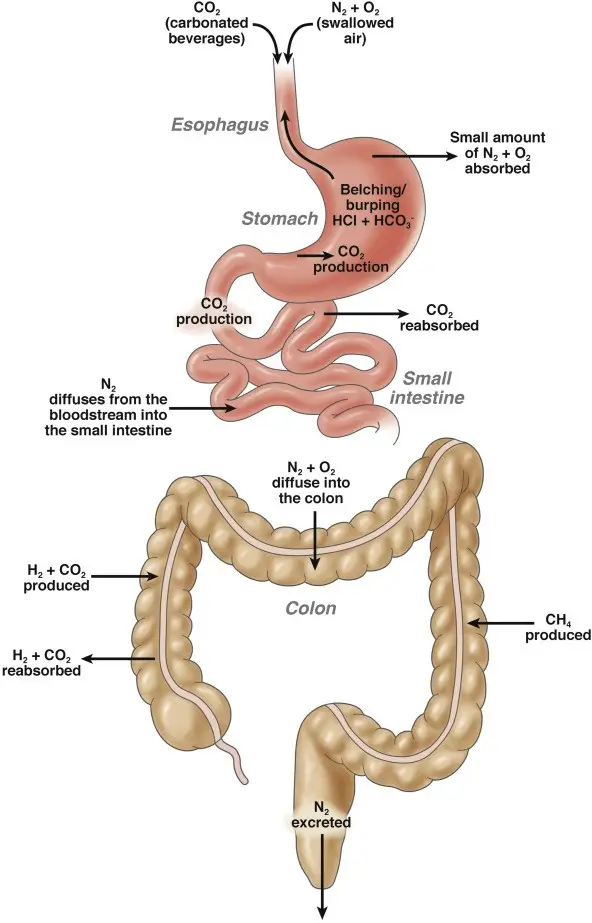
Rajah 2: Sistem penghadaman mengekalkan keseimbangan antara penghasilan, penyerapan semula, dan perkumuhan gas dengan cekap. Proses yang halus ini melibatkan pelbagai komponen penting, seumpama sebuah orkestra yang dikendalikan dengan rapi. Sebarang gangguan terhadap mekanisme ini, dalam apa jua bentuk, boleh menyebabkan penghasilan gas yang berlebihan atau pengurangan penyerapan dan penyingkiran gas, seterusnya mengakibatkan kembung (imej ihsan Lacy et al. Clinical Gastroenterology and Hepatology 2021).

Rajah 3: Imej yang menggambarkan bakteria Helicobacter pylori menjajah dinding perut dan, dari masa ke masa, menyebabkan keradangan kronik, ulser perut, serta kanser (imej ihsan laman web RACGP).
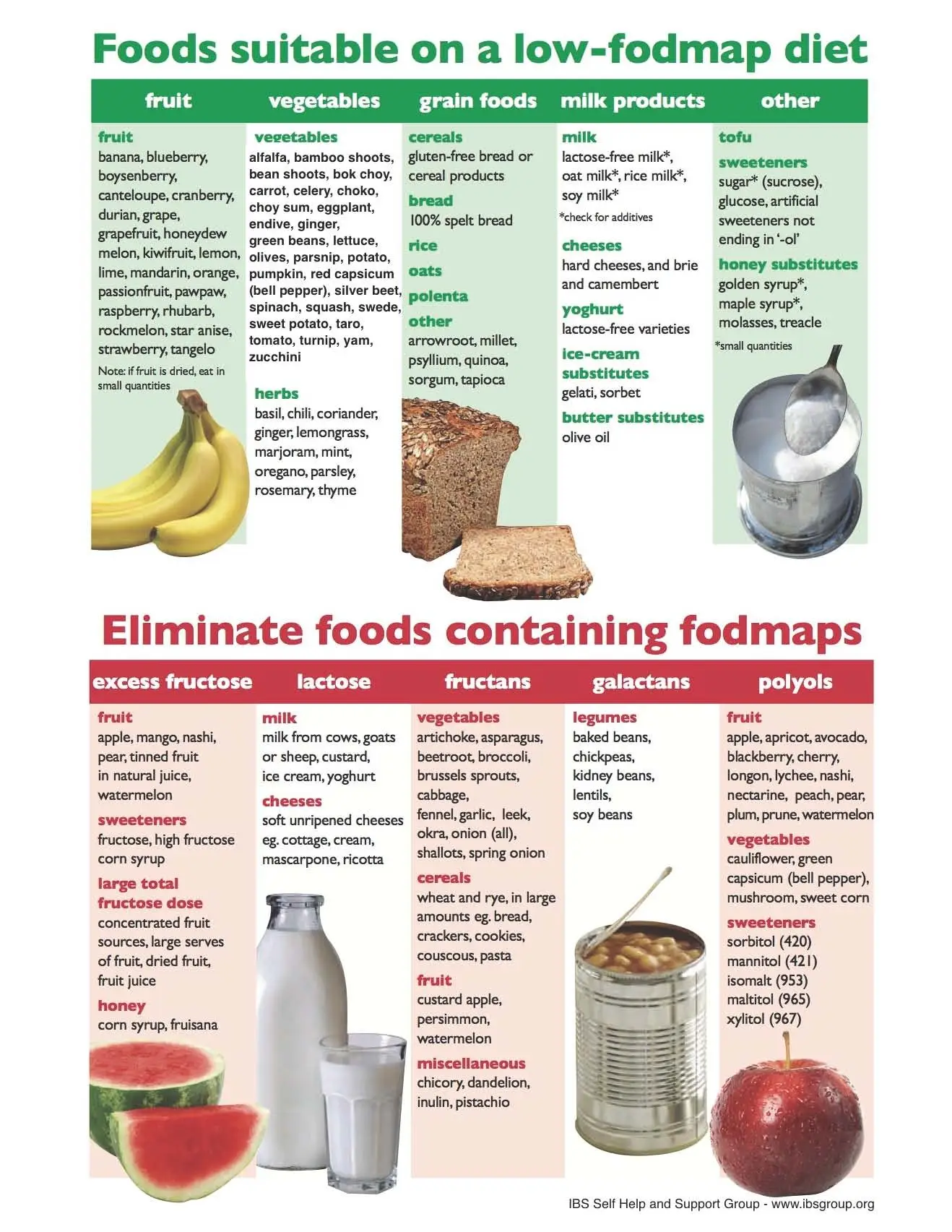
Rajah 4: Carta umum yang memaparkan kategori diet rendah dan tinggi FODMAP. Rundingan dengan pakar gastroenterologi dan pakar diet adalah disyorkan sebelum memulakan pendekatan diet ini. Selain mengamalkan diet ini secara kendiri, adalah penting untuk memahami kaedah serta masa yang sesuai bagi memperkenalkan semula makanan selepas tempoh penghapusan kumpulan makanan. Diet rendah FODMAP tidak sesuai untuk diamalkan secara jangka panjang kerana ia tidak membekalkan nutrisi yang mencukupi (imej ihsan laman web Gastroenterology Associates of New Jersey).
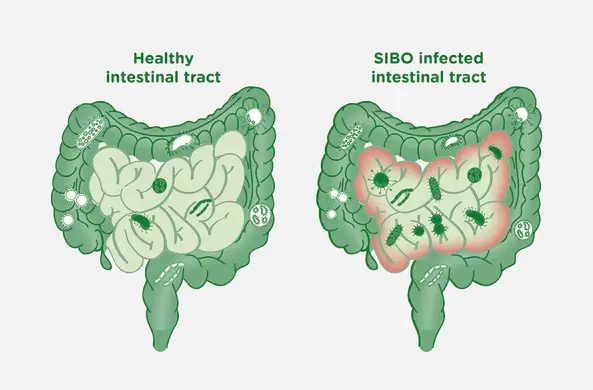
Rajah 5: Rajah ini sering saya tunjukkan kepada pesakit yang mengalami SIBO – ia menggambarkan pertumbuhan berlebihan mikroorganisma dalam usus kecil. Usus kecil lazimnya merupakan persekitaran yang bersih, disokong oleh pergerakan sapuan berterusan (peristalsis) yang membantu mengekalkan kebersihannya. Gangguan motiliti yang menjejaskan peristalsis boleh mengganggu proses ini dan seterusnya menggalakkan pertumbuhan berlebihan bakteria, lalu menyebabkan SIBO. Bakteria 'tidak baik' yang telah menetap dalam usus kecil akan terus membiak dan menghasilkan gas berbau, mengakibatkan kembung dan distensi abdomen (imej ihsan laman web BioKPlus Canada).
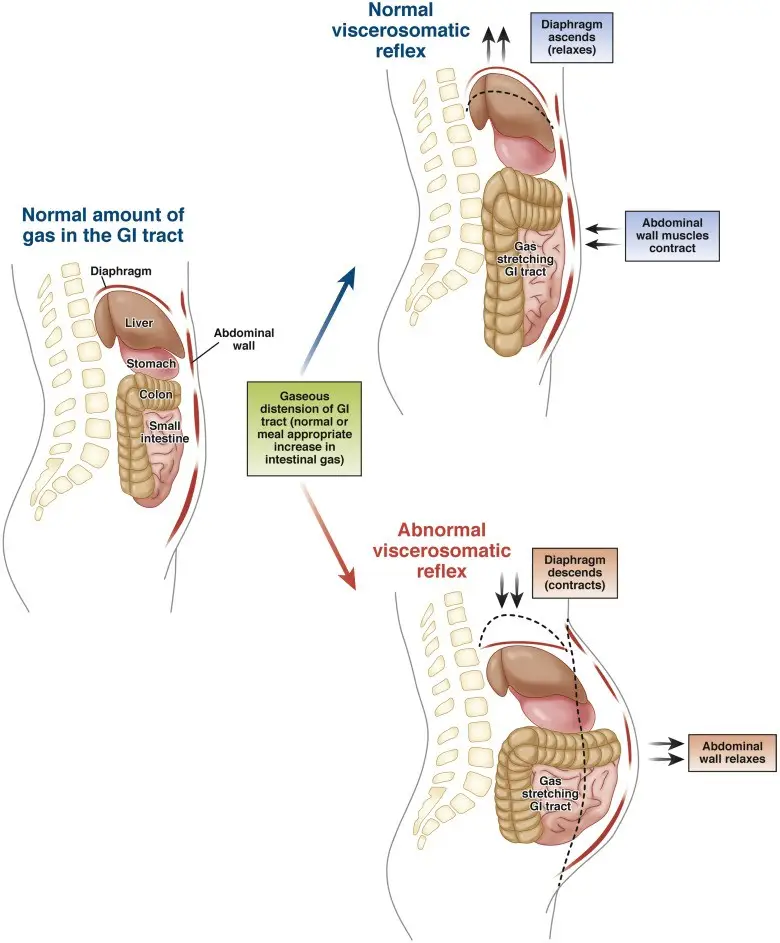
Rajah 6: Salah satu mekanisme yang dicadangkan dalam kembung fungsional melibatkan koordinasi yang lemah antara otot diafragma dan otot dinding abdomen. Dalam individu yang sihat, tubuh bertindak balas terhadap peningkatan gas dengan merehatkan diafragma dan mengecutkan otot dinding abdomen. Mekanisme ini membantu mengagihkan gas secara sekata, sekali gus mencegah pembengkakan abdomen. Namun, dalam kalangan pesakit dengan kembung fungsional, refleks ini tidak berfungsi dengan baik – diafragma berkontraksi manakala otot dinding abdomen mengendur, lalu menyebabkan kembung yang ketara serta penonjolan dinding abdomen (imej ihsan Lacy et al. Clinical Gastroenterology and Hepatology 2021).
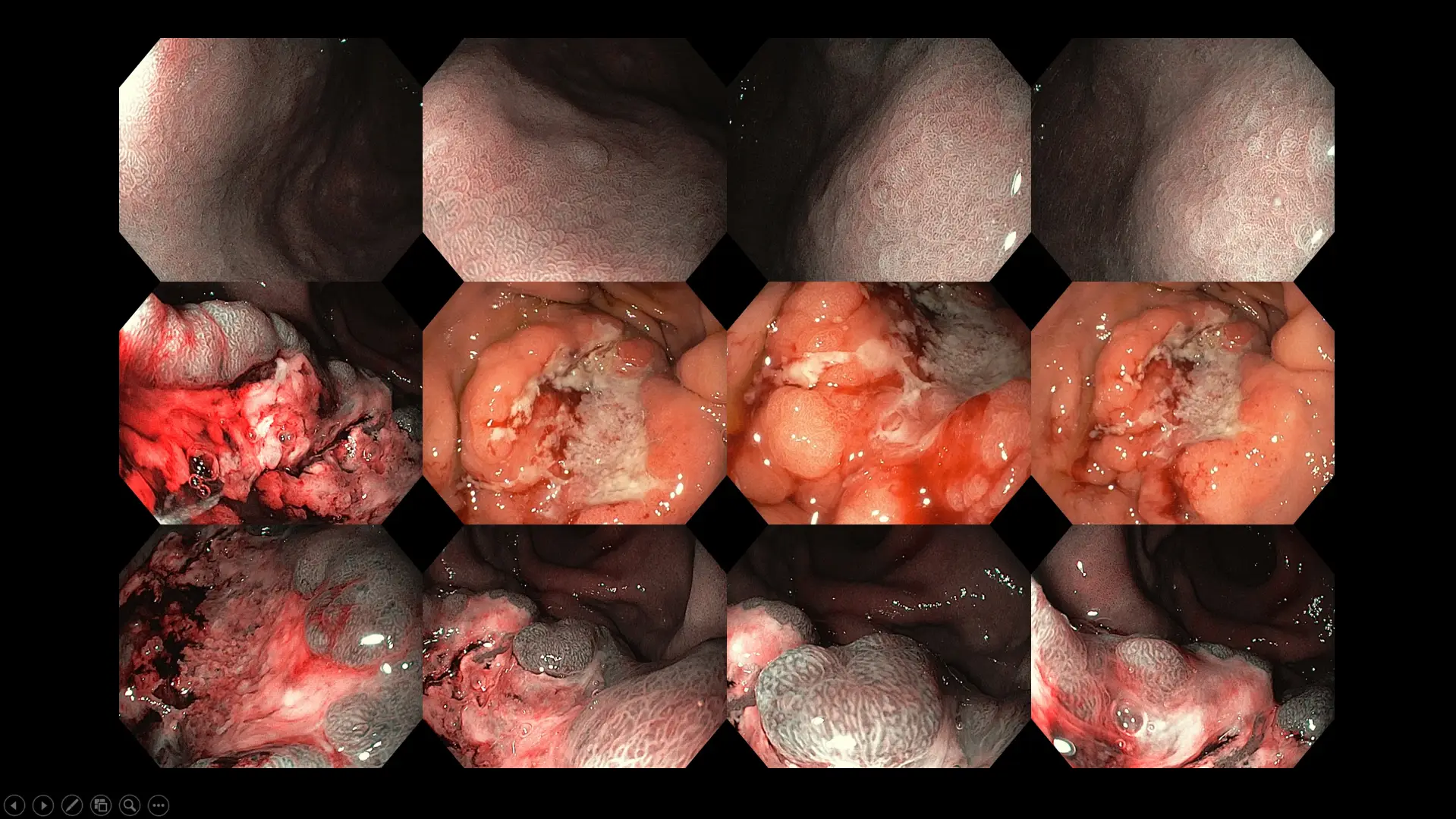
Rajah 7: Kes kanser perut peringkat lanjut berlatarbelakangkan jangkitan Helicobacter pylori – pesakit mengalami kembung, ketidakselesaan abdomen, cepat kenyang, kehilangan selera makan, dan penurunan berat badan selama tiga bulan sebelum mendapatkan rawatan.
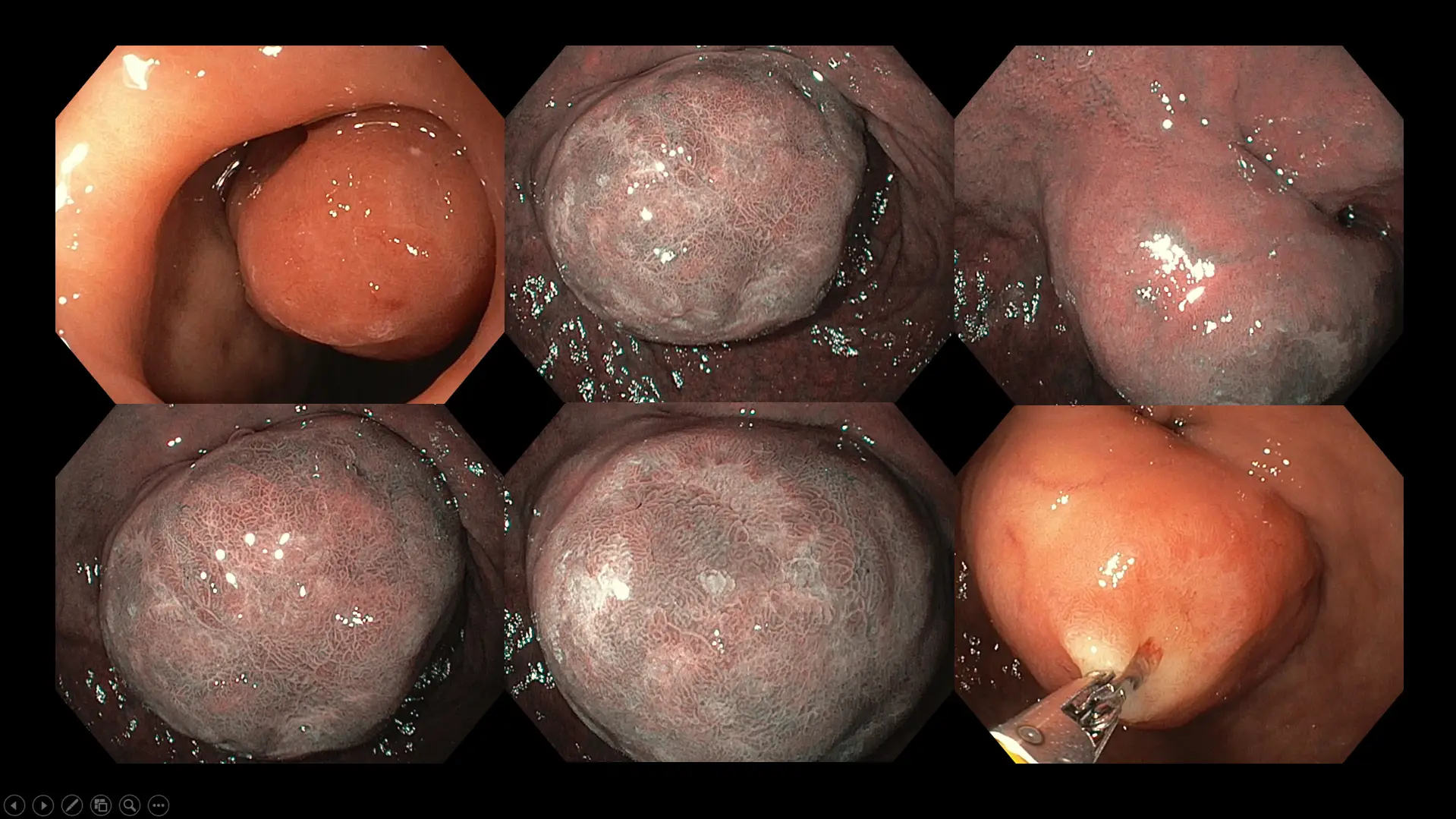
Rajah 8: Kes tumor besar pada duodenum (bahagian pertama usus kecil) dalam kalangan pesakit yang mengalami rasa penuh abdomen kronik, kembung, dan ketidakselesaan kekejangan ringan. Walaupun pembedahan penyingkiran dicadangkan berikutan saiz polip tersebut, pesakit kami memilih pendekatan konservatif tunggu dan pantau berikutan usia lanjut serta pelbagai masalah perubatan yang dihidapinya.

Rajah 9: Kes kanser kolon sebelah kiri peringkat lanjut, dengan gejala sembelit yang baru bermula dan kembung selama enam bulan sebelum pesakit berjumpa doktor.

Rajah 10: Kes yang menggambarkan penyakit divertikular usus besar dengan najis terperangkap. Pesakit kami mengalami kekejangan abdomen yang kerap beberapa jam selepas pengambilan makanan berat, disertai kembung dan sembelit. Saiz orifis divertikular adalah berbeza-beza, bermula daripada sekecil 1 mm pada sesetengah pesakit sehingga mencapai 10 cm dalam kes yang teruk.
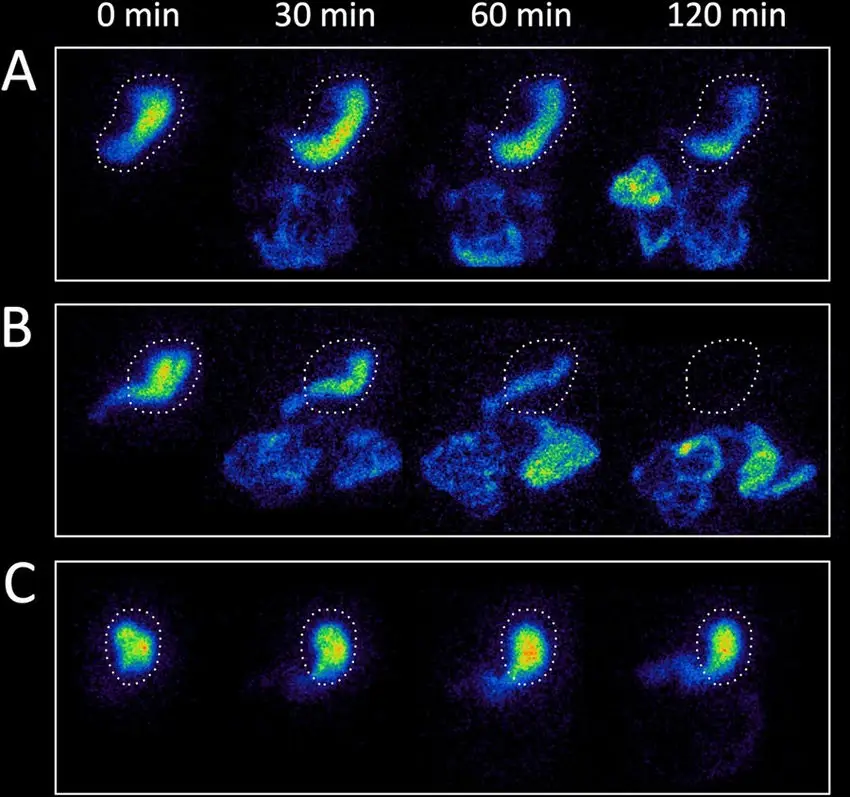
Rajah 11: Panel imej skintigrafi pengosongan gastrik bagi tiga pesakit – (A) individu sihat dengan masa pengosongan perut yang normal, (B) pesakit dengan pengosongan gastrik yang cepat selepas pengambilan ubat, (C) pesakit dengan pengosongan gastrik yang tertunda. Secara normal, perut mengosongkan 60% kandungan dalam 2 jam dan 90% dalam 4 jam. Pesakit dengan pengosongan gastrik yang tertunda akan mengalami gastroparesis, yang boleh disebabkan oleh jangkitan, pembedahan perut terdahulu yang menjejaskan saraf vagus, diabetes mellitus yang tidak terkawal sehingga mengganggu fungsi saraf autonomi yang membekalkan perut, serta gangguan neurologi dan autoimun tertentu. Dalam sebahagian kes, puncanya adalah idiopatik (tidak diketahui) (imej ihsan Borghammer et al. NPJ Parkinson’s Disease 2017).
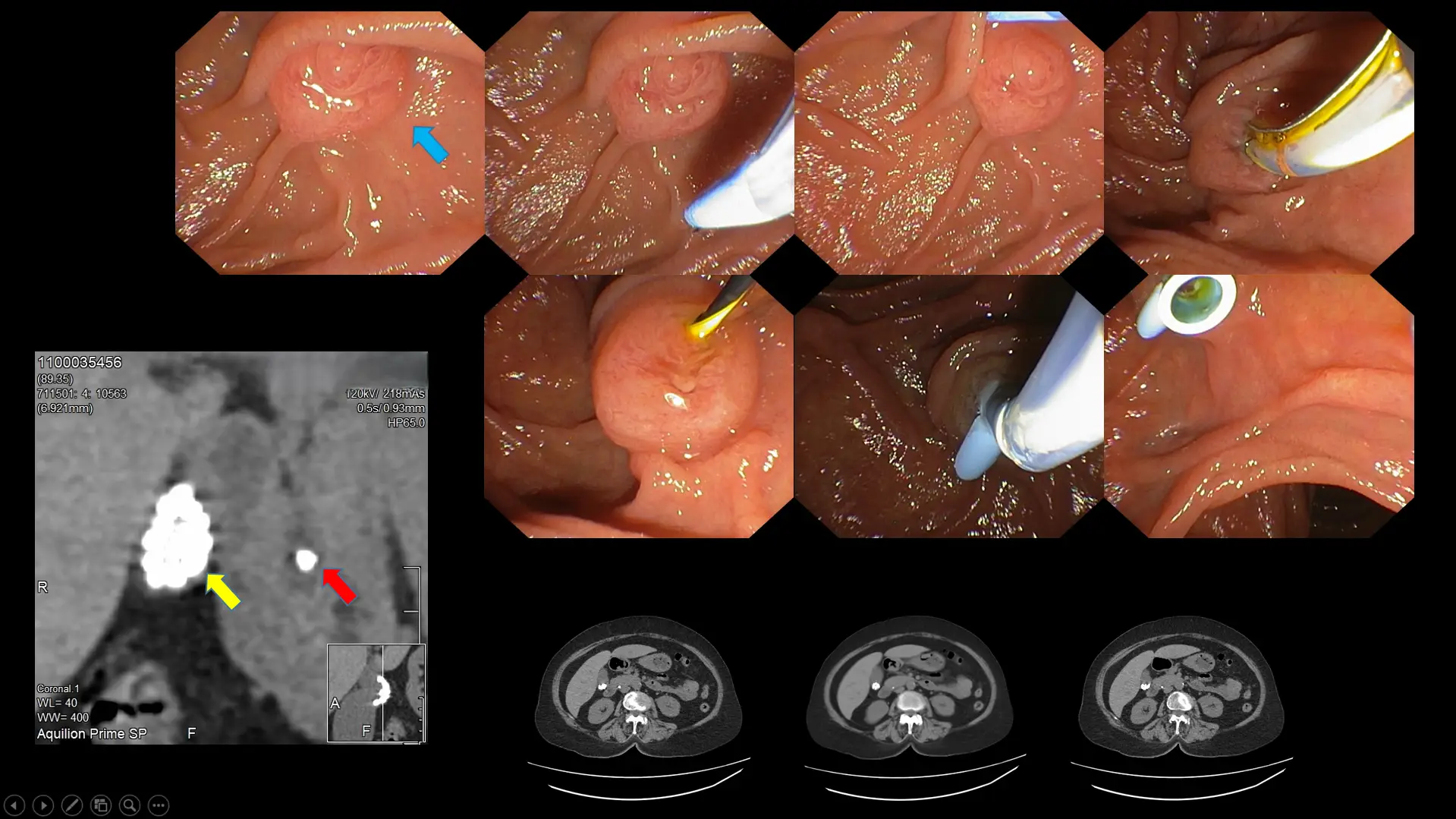
Rajah 12: Contoh pesakit dengan keradangan pundi hempedu berpanjangan yang disebabkan oleh batu pundi hempedu (anak panah kuning). Salah satu batu telah terkeluar dan tersangkut di salur hempedu (anak panah merah), mengakibatkan jangkitan serta kesakitan yang teruk akibat halangan aliran hempedu ke usus kecil (anak panah biru menunjukkan bukaan salur hempedu ke dalam usus kecil). Prosedur kolangiopankreatografi retrograd endoskopik (ERCP), telah dilakukan tepat pada masanya bagi memulihkan aliran salur hempedu melalui pemasangan tiub plastik pada bukaan berkenaan.
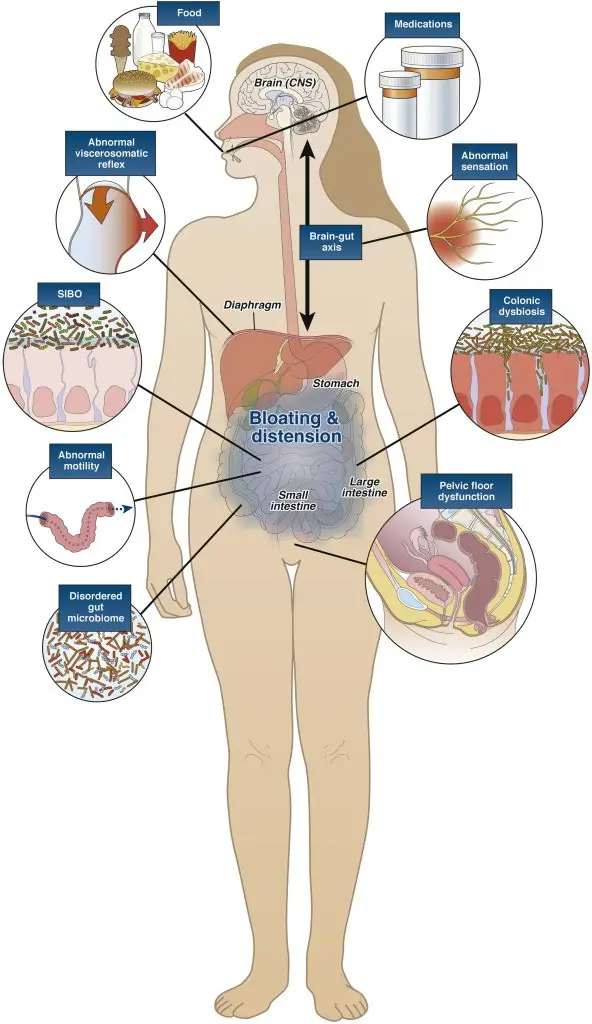
Rajah 13: Ilustrasi kartun yang merangkumkan pelbagai punca fungsional gas berlebihan dan kembung, yang paling lazim termasuk makanan dan ubat-ubatan, jangkitan gastrousus terdahulu, gangguan motiliti usus, pertumbuhan bakteria berlebihan yang membawa kepada disbiosis usus, peningkatan persepsi terhadap kesakitan dan gas akibat gangguan paksi usus–otak, serta ketidakselarasan antara otot dinding abdomen dan diafragma (imej ihsan Lacy et al. Clinical Gastroenterology and Hepatology 2021).
PEMERIKSAAN DAN UJIAN
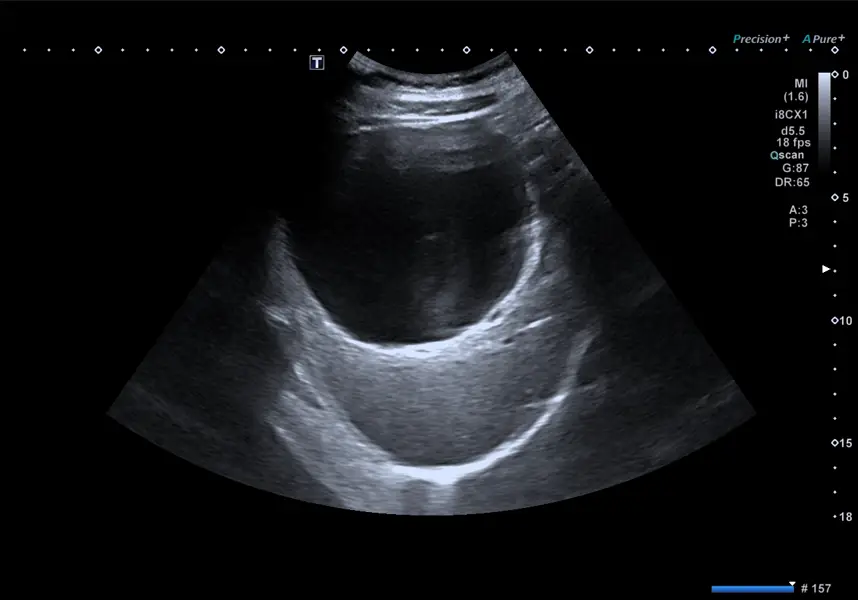
Rajah 14: Imbasan ultrabunyi abdomen yang menunjukkan sista hati besar dalam kalangan pesakit dengan gejala cepat kenyang, ketidakselesaan epigastrik, dan kembung. Ultrasonografi sering menjadi pilihan sebagai pemeriksaan awal kerana tahap keselamatannya, tidak melibatkan pendedahan radiasi, mudah didapati, mudah digunakan, dan menjimatkan kos.

Rajah 15: Imbasan CT berguna apabila penilaian yang lebih terperinci diperlukan untuk menilai patologi yang telah diketahui atau disyaki, terutamanya apabila ultrasonografi tidak mencukupi. Imbasan CT juga boleh digunakan sebagai modaliti utama apabila keganasan disyaki atau sekiranya pembedahan mungkin diperlukan pada peringkat seterusnya. Rajah di atas menunjukkan imbasan CT abdomen dan pelvis yang mendedahkan tumor ovari jinak bersaiz besar pada pesakit yang hadir dengan rasa penuh abdomen, pembengkakan, kembung, serta selera makan berkurangan.
Ujian tidak invasif hanya dipertimbangkan bagi pesakit tanpa tanda amaran, dengan pemilihan ujian bergantung kepada punca asas yang disyaki. Ujian nafas urea, sebagai contoh, digunakan untuk mengesan jangkitan Helicobacter pylori. Sebaliknya, ujian nafas hidrogen atau laktulosa digunakan untuk pesakit yang disyaki mengalami pertumbuhan bakteria berlebihan dalam usus kecil atau malabsorpsi karbohidrat. Ujian yang lebih lanjut untuk menilai gangguan motiliti termasuk manometri esofagus resolusi tinggi bagi mengenal pasti kelainan esofagus, kajian pengosongan gastrik menggunakan skintigrafi nuklear dengan kamera gama untuk mengesan gastroparesis (rujuk Rajah 11), kajian transit kolon menggunakan kapsul Sitzmarks bersama beberapa imbasan sinar-X abdomen bagi menilai masa transit usus besar, serta kajian anorektal yang menggunakan manometri anorektal resolusi tinggi untuk menilai fungsi otot dubur dan rektum.
Rajah 16: Kajian kapsul Sitzmarks merupakan alat yang praktikal, selamat, dan menjimatkan kos untuk menilai subjenis sembelit – sama ada berkaitan gangguan motiliti kolon (sembelit transit perlahan) atau disfungsi otot anorektal (defekasi disinergik). Selepas menelan kapsul tersebut, imbasan sinar-X abdomen akan dilakukan selepas lima hari untuk menilai bilangan cincin yang masih tinggal serta taburannya (imej ihsan laman web Sitzmarks.com).
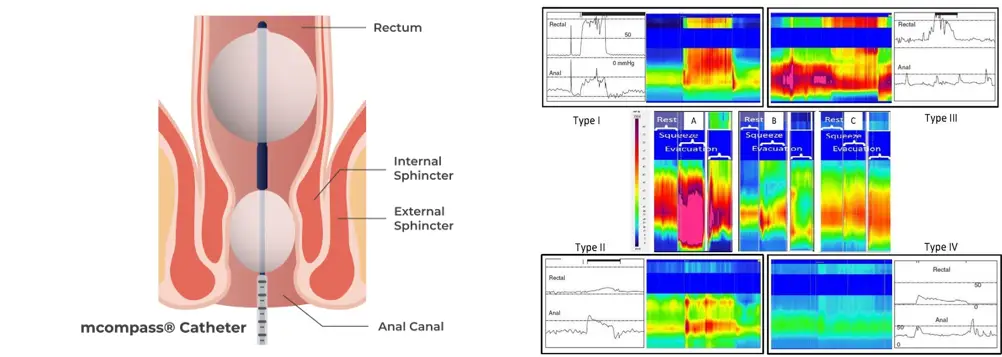
Rajah 17: Imej yang menunjukkan cara manometri anorektal dijalankan (kiri) serta analisis data yang dilakukan selepas prosedur tersebut (kanan). Penilaian sebegini membolehkan klinikal mengenal pasti subjenis sembelit yang berpunca daripada ketidakselarasan antara rektum dan otot dubur, sekali gus membantu menentukan pilihan rawatan yang paling sesuai (imej ihsan laman web Medspira dan Lee et al. Journal of Neurogastroenterology and Motility 2018).
Prinsip pengurusan bergantung kepada punca yang mendasari, dan seperti yang dapat kita lihat, kembung boleh berpunca daripada pelbagai faktor. Usaha mengenal pasti punca masalah ini sering mencabar kerana terdapat pelbagai perangkap diagnostik, khususnya punca yang bukan berkaitan gastroenterologi. Pemeriksaan yang dipilih tidak semestinya bergantung kepada satu alat piawai emas semata-mata, sebaliknya sering melibatkan gabungan beberapa ujian bagi menyokong dan mengesahkan diagnosis. Doktor anda akan membantu mengenal pasti punca sebenar, namun proses ini mungkin mengambil masa dan memerlukan beberapa lawatan serta susulan. Kesabaran dan usaha tersebut terbukti berbaloi, memandangkan kembung merupakan pengalaman yang tidak menyenangkan, dan penyelesaian yang berkesan serta tepat pada masanya amat dihargai.
Kesimpulannya, sekiranya anda mengalami gejala kembung yang mengganggu dan tidak pasti puncanya, disarankan mendapatkan penilaian perubatan di klinik berdekatan. Dalam sesetengah keadaan, keprihatinan awal lebih bermakna berbanding sikap mengambil mudah. Akhir kata, izinkan saya berkongsi mesej utama –walaupun gas boleh menyumbang kepada kembung, ia bukan satu-satunya punca.




.webp?sfvrsn=20763f7d_21)
.webp?sfvrsn=f2a2c343_12)
 +604–643 8799
+604–643 8799
 Minta temu janji
Minta temu janji.webp?sfvrsn=276ce14_1/vector-(3).webp) Pesakit Antarabangsa
Pesakit Antarabangsa.webp)